 Anatomy, Bony Pelvis and Lower Limb: Foot Dorsalis Pedis Artery
Anatomy, Bony Pelvis and Lower Limb: Foot Dorsalis Pedis Artery
Introduction
The dorsalis pedis artery (DPA) is a main artery of the foot. It is a continuation of the anterior tibial artery as it crosses the ankle joint. One of the primary functions of the DPA is to carry oxygenated blood to the dorsum of the foot.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The main arterial supply to the leg and foot is the femoral artery which passes through the adductor hiatus in the thigh to become the popliteal artery. The popliteal artery travels through the popliteal fossa on the posterior aspect of the knee joint, before ending in two main branches: the anterior tibial artery and the tibioperoneal trunk (tibial artery). The tibioperoneal trunk then branches into the posterior tibial artery, and peroneal artery. The anterior tibial artery is most commonly the first branch and courses through the interosseous membrane, continuing down the anterior compartment of the leg and running along with the deep peroneal nerve. It ultimately becomes the dorsalis pedis artery (DPA) as it crosses over the ankle joint.[1][2] The embryological development of the DPA is a complex process, and anatomical variations are not uncommon. Several reports have described the origin of the dorsalis pedis artery from the peroneal (fibular) artery and not a continuation of the anterior tibial artery.[3][4] The DPA is a significant landmark in palpating the pedal pulse on physical exam and involves reconstructive surgeries of the foot. The DPA also serves as a potential distal target for peripheral bypass surgery, used for limb salvage purposes in patients with ischemic foot complications.[5]
Embryology
During the development of the arterial system in the lower extremity, lumbar intersegmental arteries join to form the central or axial artery. This artery later anastomoses with the terminal branch of the abdominal aorta, known as the common iliac artery. As the limb bud lengthens, the axial artery becomes the sciatic artery in the thigh. The femoral artery then branches off the external iliac artery and joins the sciatic artery. The proximal part of the sciatic artery then regresses, and primitive middle and distal segments continue as the popliteal and peroneal arteries. On reaching the distal border of the popliteus muscle, branching off the popliteal artery, the anterior tibial artery arises passing ventrally between the tibia and fibula becoming the DPA.[4]
Blood Supply and Lymphatics
The peroneal (fibular), posterior tibial, and anterior tibial arteries are the three named arteries supplying the foot. The DPA is a continuation of the anterior tibial artery after it crosses the ankle joint. It runs over the dorsum of the foot, across the tarsal bones, and then dives inferiorly between the first dorsal interosseous muscle heading towards the plantar aspect of the foot. The DPA divides into a small arcuate artery and a larger deep plantar artery which branches to dorsal metatarsal arteries and terminates as small dorsal digital arteries. Two other branches of the DPA include the medial and lateral tarsal arteries.[6]
Deep and superficial veins drain the lower extremity. The deep veins drain into the tibial veins in the calf muscles, and the superficial veins drain into the great saphenous vein and small saphenous veins. The lymphatic drainage of the leg and foot enters the popliteal lymph nodes, and subsequently the superficial and deep inguinal lymph nodes.[7]
Nerves
The deep peroneal (fibular) nerve supplies the muscles on the dorsum of the foot and gives off a lateral branch and two dorsal digital nerves. The lateral branch aids in supplying the intertarsal joints and two dorsal digital nerves supply the great and the second toe. Autonomic innervation by postganglionic sympathetic nerves travels along the peripheral nerves and supplies the vascular smooth muscle of the foot. These nerve fibers cause vasoconstriction while hormones and local mediators regulate vasodilation.[6][8]
Muscles
The DPA supplies two closely associated muscles on the dorsum of the foot- the extensor hallucis brevis and the extensor digitorum brevis. The extensor hallucis brevis is the largest and most medially located muscle on the dorsum of the foot with its tendon attaching to the proximal phalanx of the great toe. The extensor digitorum brevis divides into three bellies with tendons ending at toes 2-4 to assist the extensor digitorum longus with toe extension. These muscles receive their vascular supply from the DPA and their innervation by the deep peroneal nerve.[1][6]
Physiologic Variants
Several variations to the branch patterns of the DPA exist. For instance, if the anterior tibial artery does not reach the foot, the perforating branch of the peroneal artery becomes DPA. Also, if the arcuate artery is small or missing, the lateral tarsal artery may support the dorsal metatarsal branches.[3][4][6]
Surgical Considerations
The arteries of the lower limb are prone to atherosclerotic plaques, which may lead to decreased arterial blood flow to areas of the leg or the foot. Most times, balloon angioplasty and stenting can open the artery to improve perfusion or revascularization of the ischemic leg or foot. Sometimes, for example in diabetic patients, a bypass using the DPA as a distal target, is an operation used to treat arterial insufficiency for limb preservation. [9] Another procedure using the DPA is a tissue flap that can cover defects of the distal foot post-amputation of the toes.[5]
Clinical Significance
Because the DPA is superficial and readily palpable, it is a preferred site for palpating the pedal pulse on physical examination. The pedal pulse is palpated by placing the index and third fingers lateral to the extensor hallucis longus tendon and with light compression of the dorsum of the foot, half-way between the first and second metatarsals. A diminished or absent dorsalis pedis artery pulse may show vascular insufficiency; however, due to differences in the anterior tibialis termination, some individuals may have a congenitally non-palpable pulse.[10]
A standard component of a proper vascular examination is performing an ankle-brachial index (ABI) using an inflatable BP cuff and a hand-held Doppler ultrasound device. The ABI is essential in diagnosing peripheral vascular disease and is often used as an indicator of cardiovascular mortality and morbidity. The ABI is calculated by dividing the measured systolic blood pressure in the brachial artery by systolic blood pressure in dorsalis pedis or posterior tibial artery. A value of 0.9 to 1.1 suggests a normal ABI. An ABI less than 0.9 suggests stenosis of leg arteries while an ABI greater than 1.1 may indicate atherosclerotic stiffening or vessel hardening due to calcification of the vessel wall.[10]
Other Issues
Another clinically relevant pathology of the DPA is an aneurysm, although its occurrence is rare (0.5%). When present, it is palpable as a pulsatile mass on the dorsum of the foot. DPA aneurysm can lead to restriction of ankle dorsiflexion, paresthesia, pain, localized distal ischemia, contracture, and gangrene of the toes.[11][12]
The DPA is of clinical relevance because of its surgical and nonsurgical value. It is a potential target for surgical revascularization for limb salvage and provides outflow to the foot for more proximal procedures. The DPA also allows clinicians (both surgical and non-surgical) the ability to assess vascular disease on physical examination by both palpation and utilization of the ABI.[6][10]
Media
(Click Image to Enlarge)
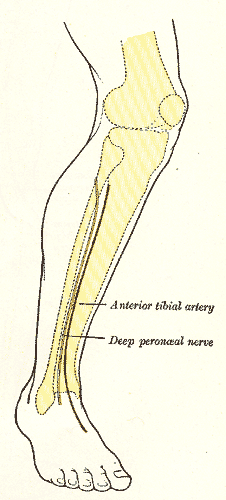
Lateral aspect of right leg; showing surface markings for bones, anterior tibial and dorsalis pedis arteries, and deep peroneal nerve
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
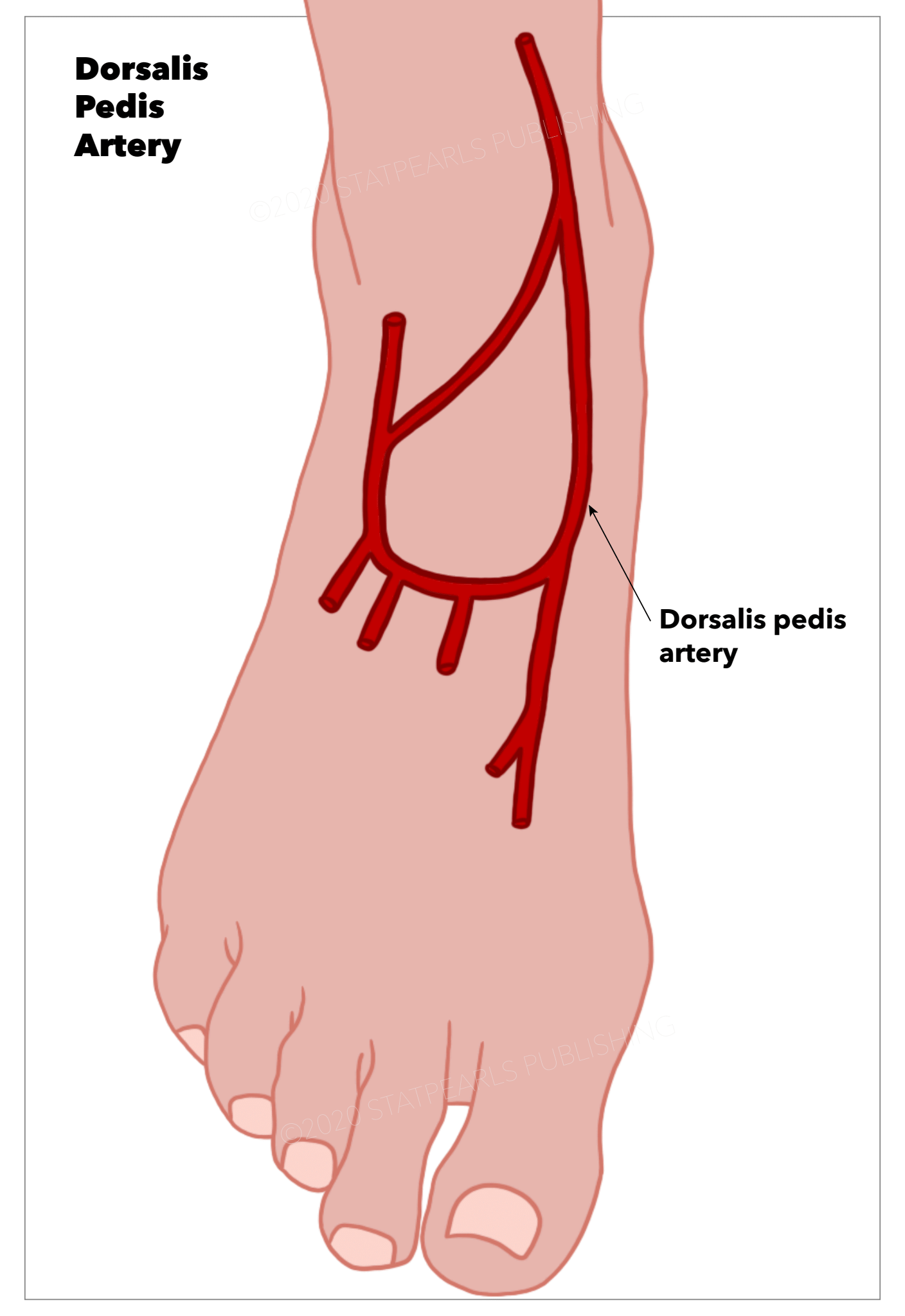
Dorsalis Pedis Artery StatPearls Publishing Illustration
References
De Maeseneer M, Madani H, Lenchik L, Kalume Brigido M, Shahabpour M, Marcelis S, de Mey J, Scafoglieri A. Normal Anatomy and Compression Areas of Nerves of the Foot and Ankle: US and MR Imaging with Anatomic Correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2015 Sep-Oct:35(5):1469-82. doi: 10.1148/rg.2015150028. Epub 2015 Aug 18 [PubMed PMID: 26284303]
Hardin JM, Devendra S. Anatomy, Bony Pelvis and Lower Limb: Calf Common Peroneal Nerve (Common Fibular Nerve). StatPearls. 2024 Jan:(): [PubMed PMID: 30422563]
Ntuli S, Nalla S, Kiter A. Anatomical variation of the Dorsalis pedis artery in a South African population - A Cadaveric Study. Foot (Edinburgh, Scotland). 2018 Jun:35():16-27. doi: 10.1016/j.foot.2018.01.002. Epub 2018 May 10 [PubMed PMID: 29753997]
Mavili E, Dönmez H, Kahriman G, Özaşlamacı A, Özcan N, Taşdemir K. Popliteal artery branching patterns detected by digital subtraction angiography. Diagnostic and interventional radiology (Ankara, Turkey). 2011 Mar:17(1):80-3. doi: 10.4261/1305-3825.DIR.3141-09.1. Epub 2010 Aug 13 [PubMed PMID: 20706978]
Pomposelli FB Jr, Marcaccio EJ, Gibbons GW, Campbell DR, Freeman DV, Burgess AM, Miller A, LoGerfo FW. Dorsalis pedis arterial bypass: durable limb salvage for foot ischemia in patients with diabetes mellitus. Journal of vascular surgery. 1995 Mar:21(3):375-84 [PubMed PMID: 7877219]
Chitra R. The relationship between the deep fibular nerve and the dorsalis pedis artery and its surgical importance. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2009 Jan-Jun:42(1):18-21. doi: 10.4103/0970-0358.53007. Epub [PubMed PMID: 19881015]
Meissner MH. Lower extremity venous anatomy. Seminars in interventional radiology. 2005 Sep:22(3):147-56. doi: 10.1055/s-2005-921948. Epub [PubMed PMID: 21326687]
Dellon AL, Höke A, Williams EH, Williams CG, Zhang Z, Rosson GD. The sympathetic innervation of the human foot. Plastic and reconstructive surgery. 2012 Apr:129(4):905-909. doi: 10.1097/PRS.0b013e3182450be8. Epub [PubMed PMID: 22456362]
Pomposelli FB, Kansal N, Hamdan AD, Belfield A, Sheahan M, Campbell DR, Skillman JJ, Logerfo FW. A decade of experience with dorsalis pedis artery bypass: analysis of outcome in more than 1000 cases. Journal of vascular surgery. 2003 Feb:37(2):307-15 [PubMed PMID: 12563200]
Level 2 (mid-level) evidenceMcDermott MM, Criqui MH. Ankle-Brachial Index Screening and Improving Peripheral Artery Disease Detection and Outcomes. JAMA. 2018 Jul 10:320(2):143-145. doi: 10.1001/jama.2018.8953. Epub [PubMed PMID: 29998324]
Ramavath AL, Cornish JA, Ganapathi M, Williams DT. Missed diagnosis of ankle pseudoaneurysm following ankle arthroscopy: a case report. Cases journal. 2009 Oct 21:2():162. doi: 10.1186/1757-1626-2-162. Epub 2009 Oct 21 [PubMed PMID: 19946533]
Level 3 (low-level) evidenceChristoforou P, Asaloumidis N, Katseni K, Kotsis T. Dorsalis Pedis Artery Aneurysm: A Case Report and Review of the Literature. Annals of vascular surgery. 2016 Jul:34():271.e5-8. doi: 10.1016/j.avsg.2015.12.011. Epub 2016 May 10 [PubMed PMID: 27174346]
Level 3 (low-level) evidence