 Autologous Fat Grafting for Facial Rejuvenation
Autologous Fat Grafting for Facial Rejuvenation
Introduction
Fat grafting is a technique in which harvested adipose tissue is injected underneath the skin for the reconstruction of traumatic, oncologic, or congenital defects. The technique may also be used for cosmetic purposes, particularly facial rejuvenation. The term "autologous fat grafting" refers to the same procedure when the fat is harvested from the person who will also receive it, which is the most common clinical scenario. Autologous fat is considered by many to be the ideal filler material for facial rejuvenation, as it is 100% biocompatible, produces a soft and natural result, and is theoretically a permanent intervention. This article focuses on the utility of this procedure for facial rejuvenation.[1]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
As the human body ages, myriad changes occur within the face. Gravity causes descent of the facial soft tissues and creates unflattering folds and shadows (e.g., nasolabial folds, tear troughs, marionette lines, etc.), contributing to an aged appearance. Furthermore, with age, patients experience decreased facial volume secondary to a combination of dermal thinning, muscular atrophy, fat volume loss, and reduction in bone thickness.[2] While gravity-related changes are traditionally addressed with resuspension procedures such as face lifting, brow lifting, midface lifting, and neck lifting, the loss of facial volume can be addressed with various filler materials, which in some instances may provide results comparable to surgical lifting. For this reason, fat grafting and dermal filler injection have recently gained popularity as adjunctive treatments to facial rejuvenation procedures.[3] A working knowledge of facial anatomy and the relationships of various structures to fascial planes is necessary to achieve good results from fat grafting and limit the risk of complications.[4]
The harvested fat, often taken from the flank, inner thigh, or abdomen, is injected into the recipient sites only after careful planning. Identifying the proper location and depth of the fat compartments to receive the grafts is critical. The major fat compartments of the face are the superficial and deep fat spaces, which are separated by the superficial musculoaponeurotic system.[5] Each of these spaces can be further divided into units within the same plane, and the selection of appropriate recipient sites requires considerable experience. The superficial fat space contains the nasolabial fat pad, the superior, inferior, and lateral orbital fat pads, the temporal and forehead fat pads, the jowl fad pad, and the medial, middle, and lateral cheek fat pads. The deep fat space is composed of the medial and lateral sub-orbicularis oculi fat pads, the sub-orbicularis oris fat pad, the deep medial and lateral cheek fat pads, and the buccal fat pad.[6] Understanding these units enables the injectors to select appropriate sites for fat transfer and determine the required volume and the optimal injection techniques and equipment.
Indications
Autologous fat grafting intended for facial rejuvenation restores volume to the face and can also revitalize skin by improving tone and texture. While fat grafting is primarily used for elective cosmetic purposes, it is also an important minimally-invasive modality employed for several reconstructive indications.
The age-related changes in the face that can be addressed with autologous fat grafting include:
- Forehead hollowing
- Deep rhytides, particularly forehead and glabellar
- Temporal hollowing
- Supraorbital hollowing
- Increased vertical length of the lower lid
- Tear trough deformity and/or deep nasojugal groove
- Malar bags
- Nasolabial folds
- Marionette lines
- Jowls or poor jawline contour
- Thin lips
- Retruded chin
Besides treating the aging face, autologous fat grafting helps address several other problems and can be performed alone or in conjunction with facial rejuvenation.[7] These indications include:
- Nasal contour irregularities
- Scars
- Burns
- Radiation dermatitis
- Human immunodeficiency virus-associated lipodystrophy
- Facial deformities (congenital, acquired, or traumatic)
- Facial asymmetry
- Flap augmentation
Contraindications
There are several circumstances in which fat grafting may not be the ideal rejuvenation method and could potentially be unsafe, particularly if a general anesthetic is to be employed. Autologous fat grafting may be contraindicated when there is a high likelihood of instability in the fat's volume, such as in cases of planned weight loss or ongoing weight gain, or if the patient has a prior history of complete or subtotal resorption of prior grafted fat. Patients undergoing fat injection for breast reconstruction or recontouring should also be aware that injected fat may form nodules or calcifications, which may subsequently appear suspicious for malignancy on future imaging.
Patients with local, regional, or systemic conditions that may affect blood flow or wound healing are also at risk of developing complications or having suboptimal outcomes. Examples include histories of extensive burn scarring, radiation therapy, keloid scarring, coagulopathies, the need for immunosuppressive medications, and other metabolic or chronic diseases.
Equipment
Autologous fat grafting requires the following equipment:
- Wetting or tumescent solution - 500 mL normal saline, 25 mL of 1 to 2% lidocaine, and 0.5 ml epinephrine (1:100,000 or 1:200,000)
- Local anesthetic (lidocaine or bupivicaine)
- Infiltration needle or cannula - used to administer local anesthesia (to cannula entry sites) and the wetting/tumescent solution (to graft harvest sites)
- Fat harvesting and donor cannulas - the Coleman type 2 (side-port cannula) is the most commonly used injection cannula. For facial injections, the cannula should be no more than 5 to 9 cm in length. The choice of the cannula, including gauge and length, depends largely upon the graft recipient area as well as upon the experience and preferences of the injector.
- Luer-lock syringes - large syringes (10 mL or 20 mL) for harvesting and several 1 mL syringes for injecting
- A closed suction machine may be used as an alternative to syringes for harvesting large volumes of fat (low power suction may be used if harvesting large amounts of fat, though this may be traumatic and affect the integrity of the harvested fat)
- Plug to seal the Luer-lock while loading fat into the injection syringes
- #11 or#15 blade scalpel - to create an entry site for harvest cannulas
- 18 ga needle - to create an entry site for fat injection
- Sterile skin markers
- Gauze
- Compression garment
- Luer to Luer connector for micro-fat and nano-fat (for skin regeneration) processing
Depending upon the method of fat processing selected (e.g., sedimentation, filtering, washing, and centrifugation), the following may be required:
- 1 mL syringes with absorbent material (e.g., non-adherent gauze) to absorb supernatant oil
- Commercial fat grafting preparation kit
- Strainer and saline
- Centrifuge (3,000 rpm for 3 min to isolate the fat and minimize trauma)
Personnel
The team performing grating may include the following members:
- Surgeon (plastic surgeon, facial plastic surgeon, otolaryngologist, etc.) or dermatologist
- Anesthesia provider
- Nursing staff
- Operating room technicians
Preparation
Informed consent should be obtained before the procedure. The patient should understand the risks, benefits, and alternatives to the procedure. It is important to manage the patient's expectations and address any questions about the procedure. Also, the potential need for future revision procedures must be discussed because a sizeable portion of patients may need augmentation in the future due to the resorption of some of the injected fat.
Pre-procedure evaluation and consultation with a physician are required to obtain clearance for the procedure. This is important because medical conditions like bleeding disorders, anemia, and certain medications like non-steroidal anti-inflammatory drugs (NSAIDs) and anticoagulants may affect the outcome of the procedure. Patients on aspirin or NSAIDs may have to hold their medications two weeks before the surgery.
Pre-procedure photographs should be obtained. The selection of potential fat donor sites should be discussed beforehand. Also, the recipient site should be examined carefully to determine the amount of fat needed for the procedure.
Before the procedure, the necessary donor and recipient sites must be prepared. In men, facial hair may need to be shaved to improve visualization. Zones of adherence within the planned harvest region are areas of fibrosis that should be avoided, as liposuction to these regions increases the risk of trauma and/or contour irregularities. These areas should be marked in advance to avoid them.[8]
Many of these procedures are performed under general anesthesia. When employing local anesthesia, nerve blocks are preferred over local infiltration because lidocaine can decrease the viability of the harvested fat and adds volume to the recipient site, making keeping track of the progress of the fat injections more challenging.
Technique or Treatment
There are three stages involved in fat grafting.[9][10][11][12] These stages are as listed:
- Fat harvesting
- Fat processing
- Fat transfer
Fat Harvesting
Fat is initially retrieved from the donor sites selected because of the presence of rich fat reservoirs. The most common donor sites are the abdomen, periumbilical area, buttocks, medial, lateral, and anterior thigh. Occasionally, if neck or submental liposuction is performed in conjunction with a facelift and autologous fat grafting is planned, the fat harvested from the neck may be used, although the other donor sites tend to provide higher quality fat that is more likely to survive and produce the desired outcome.
The first step in harvesting fat is to use a wetting or tumescent solution for adipose tissue suspension. The composition of the wetting solution for facial rejuvenation cases, which are often more limited in scope than other fat grafting cases (e.g., breast reconstruction) and may be performed under local anesthesia, may resemble the following: 500 mL normal saline, 25 mL of 2% lidocaine, 0.5 mL epinephrine (1:100,000). The solution is infiltrated into the area from which the fat will be retrieved, usually in a 1:1 ratio to the amount of fat planned to be harvested (i.e., if 50 mL of fat is to be harvested, then 50 mL of the wetting solution should be injected).
After 15 minutes of allowing the anesthetic to take effect, a stab incision is made with a scalpel. A blunt fat harvesting cannula attached either to a Luer lock syringe or a closed suction machine with low negative pressure is inserted into the donor site, and the fat is removed by a gentle back-and-forth movement. Appropriate care should be taken to adjust the technique so that minimal bleeding is produced during this process, as blood may negatively affect the fat's viability. The plunger should be drawn back just 1-2 mL to create adequate negative pressure. If a suction machine is used, it should be set at the lowest tension to lessen the shear stress on the adipocytes and thus promote viability. The repetitive movement of the harvesting cannula back and forth through the stab incision may cause abrasion or burning of the skin edges, and excising the skin edges prior to closure will often improve the appearance of the final scar.
Fat Processing
Following harvest, several additional components like oil, dead adipocytes, blood, and local anesthetic are also present in the fat solution. The presence of any of these may compromise graft uptake by promoting necrosis, inflammation, and vasoconstriction. To improve the viability of the transferred fat, processing or refining can be carried out by any of the following three methods:
- Sedimentation - Syringes are placed upright for 45 minutes to permit gravity to separate the different components. This is the most cost-effective and causes minimal damage to the adipocytes, but it is time-consuming. Typically, another procedure is performed while waiting for sedimentation to complete.
- Centrifugation - Condensed fat can be obtained using 1 to 3 minutes of centrifugation at 3,000 rpm, as recommended by Coleman. This is a quick and reliable method of separating the elements, although overly aggressive centrifuge settings may decrease graft viability.
- Washing and filtering - Fat may be cleaned and refined using a strainer or gauze. The harvested fat is placed into a strainer or non-adherent gauze, and saline is used to rinse it. This process is inexpensive and relatively quick, and the adipocyte damage is minimal; once the extra material is removed, the fat is ready to be placed into syringes for transfer.
Sedimentation and centrifugation lead to the formation of three layers. The middle layer contains graftable fat. The uppermost layer contains oil and destroyed fat cells, which can be removed with absorbent material (e.g., gauze). The lowermost layer will have water, blood, lidocaine, and epinephrine, which should also be discarded, typically by draining the syringe containing the fat.[13]
Fat Transfer
The processed middle layer is transferred to multiple 1 mL syringes, and the fat is then injected into the recipient sites. To avoid damaging the adipocytes, it is preferable to remove the plungers from the 1 mL syringes and fill the syringes from the open back rather than aspirating the fat up through the Luer-lock end of the syringe by withdrawing the plunger. A stab incision is then made to provide access to the recipient area, usually with an 18 ga needle. Stab incision location selection is focused on providing access to as many recipient sites as possible rather than hiding the incision in facial subunit borders because the puncture sites typically heal without any noticeable scarring. Once the cannula has been introduced into the target area, multiple passes of 0.1 mL are used to deliver the fat parcels. The fat should be delivered with withdrawing movements to deposit the fat with minimal resistance and prevent intravascular injection. The passes are also performed "3-dimensionally" along different vectors and at different levels, as placement in different tissue planes leads to better aesthetic outcomes. Most fat will be injected deep to the superficial musculoaponeurotic system (or temporoparietal fascia) but superficial to the periosteum.
Overcorrection is a very common practice to take into account future resorption (up to 80%) of the fat, but the evidence regarding definitive survival rates is conflicting. In general, slight overcorrection (approximately 20%) is acceptable, although it is important to realize that while 80% of patients will keep 80% of the fat injected, the remaining 20% of patients will resorb all or nearly all of the fat. Patients who do resorb most or all of their fat will likely do so again, and are, therefore, poor candidates for repeat injection, whereas patients who only resorb up to 20% are good candidates for "top-up" injections in the future if necessary. To avoid stress on the grafts, compression garments should be worn for 2 to 3 days after the procedure, though some patients may achieve better outcomes if compression garments are worn for longer periods.
The use of platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) is an emerging technique in which the processed blood of the patient may be injected along with the fat to improve the chances of graft survival.[14]
Consideration of Facial Aesthetic Units
The amount of fat injected and into which facial subunits it is injected is determined by the patient's goals and the injector's experience. The approach and technique for injections of each facial subunit are particular to the subunit, with nuanced differences in techniques and instrument use. Below are a few general points for the more commonly injected areas of the face:[15]
- Forehead, brow, and temple: These injections are subcutaneous, intramuscular, or submuscular, usually accessed via stab incisions in the hairline or lateral brow. Any ridging encountered after injection should be massaged until smooth. Severely hollow temples may require 8 to 15 mL of fat.
- Glabella/nose: The most common features to be addressed in this region include the glabellar vertical rhytids ("frown lines" or "number 11s") or a deep radix in order to camouflage a dorsal hump. However, any contour irregularity of the nose may be addressed. The cannula entry point can be in the forehead, medial eyebrow, cheek, alar base, nasal tip, or upper cutaneous lip. Various cannulas may be employed, although the 19 ga Coleman type 3 cannula is commonly used to layer the fat from the periosteum to the intradermal layers. Fat can be injected posterior to the nasal cartilage for expansion of the internal valve, to fill concavities in the radix or within a saddle deformity, or to smooth contour irregularities after rhinoplasty or trauma.[16] Regarding the glabella, one must be careful to remain superficial (some advocate intradermal injection) and avoid intravascular injection to minimize the risk of blindness and/or stroke.
- Periorbital region: This area is technically challenging, so a conservative approach is warranted for novice fat grafters. One should take care not to place too many fat parcels at a time; proceeding slowly by injecting small aliquots of fat is critical. Initial infiltration should be deep along the orbital rim, followed by another layer placed just superficial to it. To avoid palpable or visible nodules, injections should be performed deep to the orbicularis oculi muscle because the skin of the eyelid is very thin.
- Lips: Fat injected here should be placed very superficially (just beneath the mucosa) to avoid injuring the orbicularis oris muscle and labial arteries (branches of the facial artery). Cannula choice depends on injector preference; however, smaller cannulas (e.g., 22 ga Coleman cannula) are preferred to inject into the lips.
- Cheek: Placement of fat in the malar, zygomatic, and infraorbital regions superior to a ptotic cheek can help to lift the soft tissue back into a more youthful position. Two stab incisions are often required, including one lateral to the mid-nasolabial fold and another lateral to the zygomatic arch. The location of the infraorbital nerve should be marked in order to avoid nerve injury, approximately 1 cm below the orbital rim in the mid-pupillary line. Consider filling the area anterior to the auricle (lateral cheek compartment) to avoid the face appearing too full due to injections placed more medially.
- Nasolabial fold: This area is accessed via stab incisions in the lateral chin or near the oral commissures. Grafting can be performed both deep (periosteal) and superficial (subcutaneous). Still, it should remain medial to the nasolabial fold to avoid trauma to the facial artery or deepening of the nasolabial fold.
- Mandible and chin: Fat grafting to this region can be used to address a retruded chin, jowls, or poor jawline definition. To gain access to this area, stab incisions can be made along the margin of the mandible, submental area, and pre-jowl sulcus. The fat is placed by fanning the injections laterally and inferiorly, taking care to avoid damage to the facial artery where it crosses over the mandible at the gonial notch, anterior to the masseter.
Complications
Despite meticulous harvesting, processing, and grafting techniques, there exist several complications associated with fat grafting:
- Bruising, edema, and ecchymosis are the most common sequelae
- Overcorrection due to the transfer of excess fat
- Undercorrection due to transfer of an insufficient volume of fat or excessive resorption of grafted fat
- Pyogenic granulomas and cellulitis secondary to infection and/or prolonged inflammation
- Blistering
- Scarring
- Tissue bunching or palpable deformities from injections placed too superficially
- Contour irregularities and nodules or calcifications
- Pain at the donor site due to inadequate anesthesia
- Deformity at the donor site due to excessive or unequal fat harvesting or violation of a zone of adherence
- Blindness due to occlusion of the ophthalmic artery
- Stroke due to occlusion of the internal carotid artery
- Fat embolism
Graft loss and bruising can be minimized by employing atraumatic technique, which minimizes hematoma formation. Cool compresses may be helpful in the first three days after treatment to reduce ecchymosis; excessive icing can lead to vasoconstriction and risk of graft loss. Vigorous activity should be avoided for two to three weeks after the procedure.[17]
Blindness is a rare complication of fat grafting. High-pressure injection into the supratrochlear artery may cause the fat to reach the ophthalmic artery. Once the pressure is released, the fat can then embolize in an anterograde direction, and subsequent occlusion of the central retinal artery can cause blindness. Blindness resulting from fat grafting requires urgent intervention; the patient should immediately be transferred to the hospital. Timolol 0.5% drops, aspirin 325 mg, and acetazolamide 500 mg should be administered while awaiting transfer. In addition to blindness, fat embolism may cause stroke, including headaches, nausea, vomiting, dizziness, numbness, weakness, and vital sign instability.
Facial swelling and bruises are also quite common after fat grafting. It is important to distinguish expected edema from cellulitis, which presents with fever, warmth, erythema, and tenderness. In contrast to cellulitis, edema is self-limited but may be prolonged due to the rich vascularity of the face. Prolonged edema is treated with facial lymphatic massage, therapeutic ultrasound, explaining to the patient the protracted nature of symptoms, and offering reassurance. In cases of overcorrection with fat injections that do not resorb sufficiently, the excess volume may be addressed with deoxycholic acid injection.
Clinical Significance
The face, in many ways, defines an individual's identity, and an attractive face promotes self-esteem, trustworthiness, approachability, and even personal success. Autologous fat grafting represents a powerful entry into the reconstructive surgeon's armamentarium for facial rejuvenation. In addition to its volumizing effects and skin quality benefits, autologous facial fat remains the filler choice for facial rejuvenation due to its longevity, cost-effectiveness, biocompatibility, minimal risk profile, and satisfaction rates compared to other materials.[18][19][20]
Enhancing Healthcare Team Outcomes
Autologous fat grafting is a multi-stage process that includes evaluating recipient and donor areas and fat harvesting, processing, and reinjection. Oversights, errors, or omissions during any of these steps may adversely affect the outcome. Because each patient and procedure are unique, the physician must communicate specific equipment needs, such as cannulae and instrumentation for harvesting, processing, and transfer, to the operative team before the procedure. Nurses and other team members should be able to effectively communicate expectations for the procedure and possible complications with the patient. Any misconceptions or confusion on the part of the patient must be resolved prior to the procedure.[21]
Imaging, if obtained, should be discussed with a radiologist to clarify any anatomical anomalies. This collaboration is essential for patients with histories of facial trauma or other pathology. When fat grafting is a part of complex surgery like facial reconstruction, cooperation with maxillofacial surgeons, orthopedic surgeons, orthodontists, and interventional radiologists may be necessary. [Level 5]
Nursing, Allied Health, and Interprofessional Team Interventions
- Using a compression garment is essential because the mobility of the grafted fat may cause volume loss.
- The patient should avoid massaging the grafted area in the early post-treatment phase, as doing so can shift the grafted fat.
- Applying a warm compress may improve blood flow to the grafted fat but will likely worsen edema. A cool compress may decrease swelling, but cold compresses should be avoided because of the risk of graft compromise.
- As part of the preprocedural counseling process, risks and warning signs of complications such as blindness, fat embolism, infection, and keloid formation should be discussed with the patient to facilitate early identification and intervention.
Media
(Click Image to Enlarge)
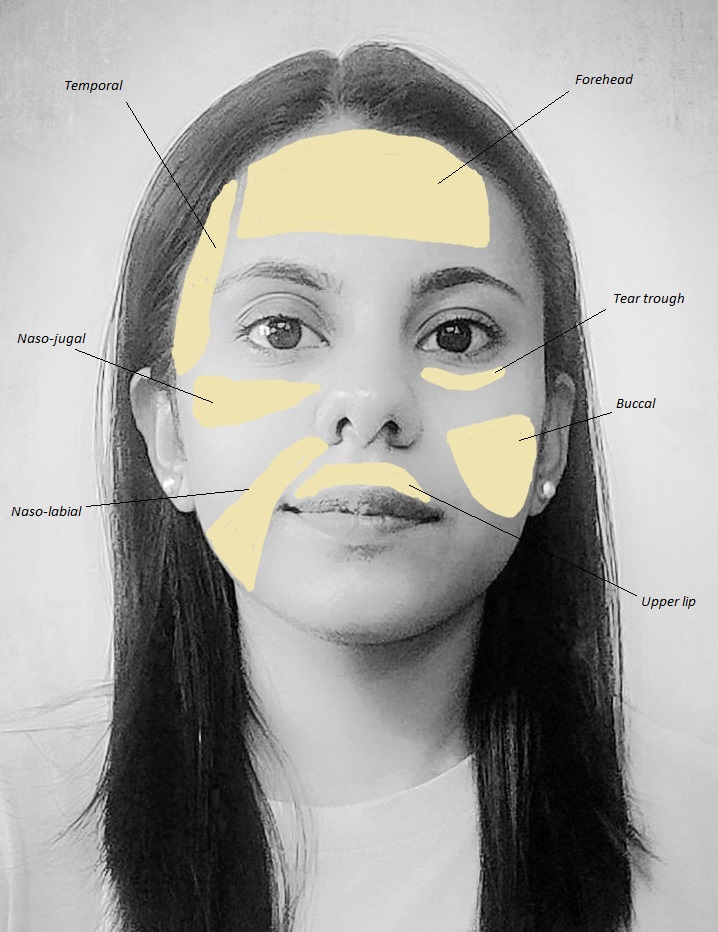
Most common areas of face used for fat grafting Contributed by Manisha A Jain, MBBS (used with permission)
(Click Image to Enlarge)
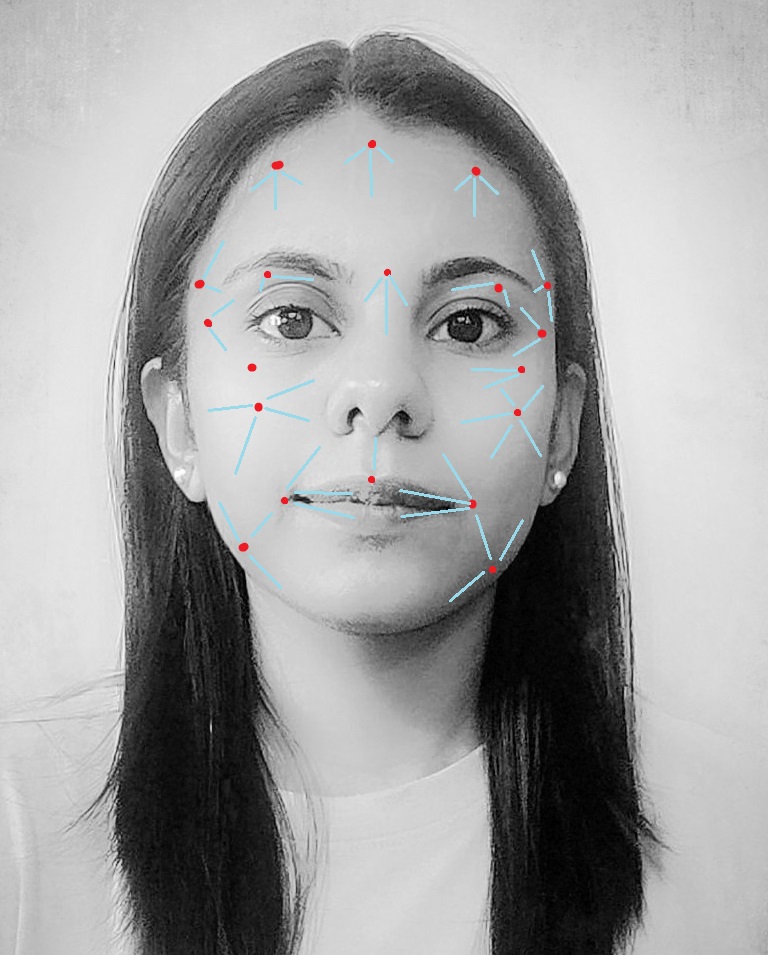
Most common injection sites and direction for fat grafting on the face. Red dots denote the injection sites and blue lines indicate the direction of the injected fat Contributed by Manisha A Jain, MBBS (used with permission)
References
Bohluli B, Bagheri SC, Consky EK. Fat Grafting as an Adjunct to Facial Rejuvenation Procedures. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):51-57. doi: 10.1016/j.cxom.2017.10.005. Epub [PubMed PMID: 29362071]
Cotofana S, Fratila AA, Schenck TL, Redka-Swoboda W, Zilinsky I, Pavicic T. The Anatomy of the Aging Face: A Review. Facial plastic surgery : FPS. 2016 Jun:32(3):253-60. doi: 10.1055/s-0036-1582234. Epub 2016 Jun 1 [PubMed PMID: 27248022]
Coleman SR, Katzel EB. Fat Grafting for Facial Filling and Regeneration. Clinics in plastic surgery. 2015 Jul:42(3):289-300, vii. doi: 10.1016/j.cps.2015.04.001. Epub [PubMed PMID: 26116934]
Frame JD. The Past, Present, and Future of Facial Fat Grafting. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):1-6. doi: 10.1016/j.cxom.2017.11.004. Epub 2017 Dec 7 [PubMed PMID: 29362066]
Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plastic and reconstructive surgery. 2007 Jun:119(7):2219-2227. doi: 10.1097/01.prs.0000265403.66886.54. Epub [PubMed PMID: 17519724]
Ramanadham SR, Rohrich RJ. Newer Understanding of Specific Anatomic Targets in the Aging Face as Applied to Injectables: Superficial and Deep Facial Fat Compartments--An Evolving Target for Site-Specific Facial Augmentation. Plastic and reconstructive surgery. 2015 Nov:136(5 Suppl):49S-55S. doi: 10.1097/PRS.0000000000001730. Epub [PubMed PMID: 26441111]
Level 3 (low-level) evidenceDiepenbrock RM, Green JM 3rd. Autologous Fat Transfer for Maxillofacial Reconstruction. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):59-68. doi: 10.1016/j.cxom.2017.11.002. Epub 2017 Dec 8 [PubMed PMID: 29362072]
Rohrich RJ, Smith PD, Marcantonio DR, Kenkel JM. The zones of adherence: role in minimizing and preventing contour deformities in liposuction. Plastic and reconstructive surgery. 2001 May:107(6):1562-9 [PubMed PMID: 11335837]
Level 3 (low-level) evidenceSimonacci F, Bertozzi N, Grieco MP, Grignaffini E, Raposio E. Procedure, applications, and outcomes of autologous fat grafting. Annals of medicine and surgery (2012). 2017 Aug:20():49-60. doi: 10.1016/j.amsu.2017.06.059. Epub 2017 Jun 27 [PubMed PMID: 28702187]
Egro FM, Coleman SR. Facial Fat Grafting: The Past, Present, and Future. Clinics in plastic surgery. 2020 Jan:47(1):1-6. doi: 10.1016/j.cps.2019.08.004. Epub 2019 Oct 21 [PubMed PMID: 31739886]
Schultz KP, Raghuram A, Davis MJ, Abu-Ghname A, Chamata E, Rohrich RJ. Fat Grafting for Facial Rejuvenation. Seminars in plastic surgery. 2020 Feb:34(1):30-37. doi: 10.1055/s-0039-3402767. Epub 2020 Feb 15 [PubMed PMID: 32071577]
Marten TJ, Elyassnia D. Fat grafting in facial rejuvenation. Clinics in plastic surgery. 2015 Apr:42(2):219-52. doi: 10.1016/j.cps.2014.12.003. Epub [PubMed PMID: 25827566]
Bagheri SC, Bohluli B, Consky EK. Current Techniques in Fat Grafting. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):7-13. doi: 10.1016/j.cxom.2017.11.001. Epub 2017 Dec 8 [PubMed PMID: 29362074]
Sarkarat F, Kahali R. Fat Graft with Growth Factors. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):33-39. doi: 10.1016/j.cxom.2017.10.003. Epub 2017 Dec 15 [PubMed PMID: 29362069]
Khan HA, Keyhan SO. Fat Grafting in Facial Aesthetic Units. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):15-23. doi: 10.1016/j.cxom.2017.10.001. Epub 2017 Dec 8 [PubMed PMID: 29362067]
Raggio BS, Asaria J. Nonsurgical Rhinoplasty Using Fillers. StatPearls. 2025 Jan:(): [PubMed PMID: 32119468]
Cuzalina A, Guerrero AV. Complications in Fat Grafting. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):77-80. doi: 10.1016/j.cxom.2017.11.003. Epub 2017 Dec 19 [PubMed PMID: 29362075]
Obagi S, Willis C. Autologous Fat Augmentation of the Face. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):41-50. doi: 10.1016/j.cxom.2017.10.004. Epub 2017 Dec 8 [PubMed PMID: 29362070]
Groen JW, Krastev TK, Hommes J, Wilschut JA, Ritt MJPF, van der Hulst RRJW. Autologous Fat Transfer for Facial Rejuvenation: A Systematic Review on Technique, Efficacy, and Satisfaction. Plastic and reconstructive surgery. Global open. 2017 Dec:5(12):e1606. doi: 10.1097/GOX.0000000000001606. Epub 2017 Dec 22 [PubMed PMID: 29632784]
Level 1 (high-level) evidenceKrastev TK, Beugels J, Hommes J, Piatkowski A, Mathijssen I, van der Hulst R. Efficacy and Safety of Autologous Fat Transfer in Facial Reconstructive Surgery: A Systematic Review and Meta-analysis. JAMA facial plastic surgery. 2018 Sep 1:20(5):351-360. doi: 10.1001/jamafacial.2018.0102. Epub [PubMed PMID: 29596574]
Level 1 (high-level) evidenceColeman SR, Lam S, Cohen SR, Bohluli B, Nahai F. Fat Grafting: Challenges and Debates. Atlas of the oral and maxillofacial surgery clinics of North America. 2018 Mar:26(1):81-84. doi: 10.1016/j.cxom.2017.10.006. Epub [PubMed PMID: 29362076]
Strong AL, Rohrich RJ, Tonnard PL, Vargo JD, Cederna PS. Technical Precision with Autologous Fat Grafting for Facial Rejuvenation: A Review of the Evolving Science. Plastic and reconstructive surgery. 2024 Feb 1:153(2):360-377. doi: 10.1097/PRS.0000000000010643. Epub 2023 May 9 [PubMed PMID: 37159906]