Introduction
Hemorrhage is an acute loss of blood from a damaged blood vessel. The bleeding can be minor, such as when the superficial vessels in the skin are damaged, leading to petechiae and ecchymosis. It can also be significant, leading to a more ambiguous constellation of symptoms, including fluctuations in vital signs and altered mental status. Hemorrhaging can be either external or internal. External bleeding occurs from a body orifice or a traumatic wound. Internal bleeding requires a high level of clinical suspicion obtained through a thorough history and physical, laboratory tests, imaging, and close monitoring of vital signs. Hemorrhage is a leading cause of potentially preventable death, especially in the acute trauma population.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The presentation of hemorrhage varies by anatomic location. After acute trauma, hemorrhage can subdivide into several anatomic areas: external wounds, bleeding within the skull, chest cavity, abdominal cavity, retroperitoneum, and from long bone fractures. A thorough history and physical is the first step in locating the source and etiology of a hemorrhage.
Hemorrhaging within the brain occurs when a vessel is ruptured and bleeds into or around the brain. The signs and symptoms will correlate with the location. The term for any bleeding occurring within the skull is an intracranial hemorrhage; this commonly occurs as a result of chronically elevated blood pressure, leading to a weakening of the arterial walls.[1] Symptoms vary, ranging from unilateral weakness to headache, nausea, vomiting, and altered mental status. Other causes of intracranial hemorrhage include heavy alcohol use, long-term tobacco use, old age, and drug abuse.[2] Trauma is another major contributor to intracranial bleeding. Another type of intracranial bleeding is a subarachnoid hemorrhage (SAH). This type of bleeding occurs due to the rupture of a bridging cortical vein, causing blood to accumulate between the delicate arachnoid mater and pia tissue, causing direct irritation to the meninges lining the brain, and can result in severe pain. The classic scenario is a patient presenting with the sudden onset of the "worst headache of their life," otherwise known as a "thunderclap headache." Ruptured aneurysms account for most cases of subarachnoid hemorrhage, but other causes include a traumatic head injury or arteriovenous malformations.[3] Additional types of intracranial bleeding include intraparenchymal hemorrhage, subdural hematoma, and epidural hematoma. Patients may present with more than one type of intracranial bleeding, especially after trauma.
Bleeding in the pleural cavity of the chest is called hemothorax. Blood enters a small space between the visceral and parietal pleura, causing the buildup of blood to interfere with normal lung expansion, ultimately affecting the transfer of oxygen and carbon dioxide between alveoli and blood. This type of breed commonly presents in traumatic injuries, metastatic cancer, blood clotting disorders, or rarely spontaneously. Symptoms include dizziness, shortness of breath, and chest pain. If bleeding continues unabated, this can result in shock or even death. If the pressure builds within the chest and affects the cardiac return of blood, this is known as a tension hemothorax, and this, too, can result in death if not treated promptly.
Traumatic blood loss in the abdomen requires a high degree of clinical suspicion. If present, symptoms can be nonspecific and usually require imaging for diagnosis. Symptoms include abdominal pain, hematemesis, hematuria, melena, and bruising, amongst others. More severe bleeding can result in hemorrhagic shock and even death. Common sources of hemorrhage include organ damage (hepatic, splenic, renal, adrenal), vascular injury, gynecologic/obstetric procedure complications, or coagulopathies. Ectopic pregnancy and cyst rupture are two common causes of an abdominal hemorrhage in a woman of childbearing age.[4]
The retroperitoneum contains visceral and vascular structures and is susceptible to injury in abdominal or pelvic injuries. The types of hematomas that develop divide into anatomic zones. Zone 1 is in a central location, and damage here includes pancreaticoduodenal injuries or major blood vessels such as the renal artery or aorta. Zone 2 involves the flanks and peri-nephric regions, including the colon. Zone 3 is the pelvic zone. An injury here is common with a pelvic fracture or femoral vascular access injuries.[5] Signs and symptoms include abdominal pain, back pain, flank pain, urinary symptoms if compressing the bladder, and femoral nerve palsy. Unique physical exam findings related to the retroperitoneum include the Grey Turner sign (bruising on the flanks).
Bone fractures can lead to dangerously fast, life-threatening hemorrhaging. The center of the long bones contains the bone marrow, where the red blood cells are made, and many arteries. The most vascular bones include the long bones: humerus, radius, ulna, femur, fibula, pelvis, and vertebrae.[6] For example, the thigh can hold up to 1 to 2 liters of blood. Trauma to blood vessels outside of the bone, but coursing with it anatomically, can also result in significant hemorrhage if they are injured. Hemorrhage can occur as a result of either a traumatic injury or during surgical repair.
Epidemiology
In Americans up to age 46, hemorrhage secondary to trauma is the leading cause of death.[7] The etiology of hemorrhage is diverse and varies by lifestyle and socioeconomic background. In 2000, the World Health Organization estimated that injury was responsible for 9% of the global mortality, and worldwide, it comprised 12% of the disease burden.[8] Approximately 90% of injuries occur in low and middle-income nations. Traffic accidents and violence contribute to high rates of fatal hemorrhages.[9]
Pathophysiology
In a healthy adult, there is an average of 4.5 to 5.5 liters or 70 to 90 ml/kg of blood circulating at any given time. Most adults can tolerate losing up to 14% of their blood volume without physical symptoms or deviations in their vital signs. The severity of hemorrhage is divided into a class system organized by the percent of blood volume loss. Up to 15% of blood volume loss classifies as a Class I hemorrhage. The patient is generally asymptomatic, and vital signs are within normal limits. Class II hemorrhage is a loss of 15 to 30% of total blood volume. Common manifestations include complaints of nausea and fatigue. On physical exam, there will be pallor and cooling of the extremities. Vital signs will start to deviate from normal, with tachycardia being the first vital sign to increase (100 to 120 beats per minute), followed by an increased respiratory rate (20-24 breaths per minute). Class III hemorrhage is 30 to 40% of total blood volume loss. Common manifestations include delayed capillary refill (greater than two seconds) and changes in mental status. Drastic blood pressure deviations (less than 90 mm Hg) are generally not seen until 30% of the blood volume is lost. Vital signs may reflect a systolic less than 90 mmHg or 20 to 30% of original measurement; HR is greater than 120; changes in mental status; and narrow pulse pressure (less than 25 mm Hg). These changes represent the body attempting to maintain perfusion to the vital organs by constricting peripheral blood vessels. Class IV hemorrhage is defined as greater than 40% of total blood volume loss. There is commonly a lack of urine output, absent peripheral pulses, and further deviations in vital signs. Severe hemorrhaging can lead to shock, which occurs when the blood loss becomes significant enough that it is unable to meet the oxygen demands of the tissue. Cellular aerobic metabolism shuts down, and anaerobic metabolism begins, leading to the production of lactic acid and, ultimately, metabolic acidosis.[10] The risk is very high for organ failure, coma, and death, absent the timely implementation of life-saving interventions.
History and Physical
History and physical exams are essential in the pursuit of a source of hemorrhage. Information regarding the history of present illness, including the mechanism of injury if traumatic, may help the health care provider start to narrow in on a site(s) of hemorrhage. The traditional teaching in the evaluation of a trauma patient includes primary and secondary surveys. One of the key components of the initial survey is "C," which stands for circulation. This evaluation includes both an assessment and, where feasible, an attempt to control significant hemorrhage. When evaluating after trauma, the health care provider should remember there are five areas where a patient can have a potentially life-threatening hemorrhage: externally, the thorax, the abdomen, the retroperitoneum, the pelvis, and the thighs.
Important history to obtain in a patient with concerns for hemorrhage includes the use of any anticoagulant or antiplatelet medications, history of any bleeding diathesis, or recent trauma or procedures. Gastrointestinal hemorrhage may be difficult to identify a source without further imaging or procedure, but a good history is essential, and a thorough physical exam can lead to clues as to the source of the hemorrhage.
Intracranial hemorrhage evaluation should also start with a thorough history and physical exam. Often, this can lead a provider to suspect a specific etiology or type of bleed, but imaging is often necessary to confirm these suspicions.
Nontraumatic hemorrhage will be evidenced by tachycardia, hypotension, hematochezia, melena, hemoptysis, or hematuria.
Evaluation
Aside from a thorough history and physical, the workup will likely require imaging and laboratory tests. For a bleed in the skull, a prompt, non-contrast CT scan is necessary within six hours of onset for the best outcomes.[11] MRI is considered to be more sensitive as time passes the six-hour threshold.[12] A lumbar puncture is another useful diagnostic test as it can reveal the presence of RBCs in the CSF or xanthochromia, indicating hemorrhage.
For bleeding in the chest, diagnosis is aided using a chest X-ray, ultrasound, or CT scan, depending on the available resources (and the patient's clinical stability). Hemodynamically unstable patients should not be moved to a diagnostic area for evaluation. Bedside procedures such as chest X-ray and/or ultrasound can help make a diagnosis of a significant hemothorax without moving the patient to a more uncontrolled area, such as is often required for advanced imaging like a CT scan. A fluid analysis will definitively diagnose the presence of blood from other forms of fluid. Treatment includes placement of a chest tube for drainage and possible surgical exploration if there is greater than 1500 mL output initially or greater than 200 mL per hour after initial placement.
Especially in the setting of shock secondary to abdominal bleeding, the use of a CT scan and the focused assessment with sonography for trauma (FAST Scan) are indicated.[13][14] A FAST is a highly reliable, noninvasive diagnostic test available at the bedside. For example, it can be used to assess for an abdominal aortic aneurysm in a patient with concerning symptoms.[15] Indications for surgical intervention in those with suspected abdominal bleeding include peritoneal signs, clinical deterioration, hemodynamic instability, and a positive FAST exam. Patients with hemodynamic stability should undergo less invasive methods of imaging before surgical intervention, as indicated. Retroperitoneal bleeds can undergo an evaluation with a CT scan and ultrasound.[5]
Evaluation of bleeding from an anatomic orifice often relies on endoscopy of the area of concern, which may include but is not limited to bronchoscopy, cystoscopy, colonoscopy, or esophagogastroduodenoscopy (EGD).
Treatment / Management
The management of hemorrhage will vary based on anatomic location, the extent of the injury, patient presentation, and the resources available. Resuscitation with IV fluids is necessary if the patient is demonstrating signs of hypovolemia. Basic fluid resuscitation is by placing two large bore IVs, infusing normal saline or lactated ringer, and beginning transfusion protocol. Blood product administration should be in equivalent amounts (1:1:1 PRBCs, FFP, platelets) and transfused as needed. Patients receiving transfusions should have monitoring for hypothermia. The goals of treatment are to restore intravascular volume and to maintain oxygen delivery until the source of bleeding can be resolved. Target mean arterial pressure (MAP) is a pressure greater than 65 mm Hg. For penetrating trauma, a systolic blood pressure goal is greater than 90mmHg. For brain injuries, the goal MAP is 105 mm Hg or higher and SBP greater than 120 mm Hg.[16] It is also essential to monitor lactic acid production and worsening metabolic acidosis as this can lead to loss of peripheral vasoconstriction and cardiovascular collapse. For traumatic external wounds, direct pressure and placement of tourniquets proximal to the source of the hemorrhage can be life-saving interventions.
Differential Diagnosis
Prompt detection of a bleed requires an astute clinician. A thorough history and physical will raise suspicion and require timely intervention. Some forms of hemorrhage will present due to hypovolemia, and this can result in hypovolemic shock. Care must be taken to distinguish this entity from other etiologies of shock. Other bleeds, such as those in the brain, have little room for the excess blood to accumulate before pressures rise and evoke mental status and neurological changes. Other differentials to consider are migraine headaches, meningitis/encephalitis, tumors, electrolyte abnormalities, stroke, myocardial infarction, and intoxication/poisoning, to name a few.
Prognosis
Prognosis is dependent upon early detection and timely intervention. Mortality in traumatic wounds leading to hemorrhagic shock is high. The role of the physician is to maintain oxygen delivery, control the bleeding, and limit tissue hypoxia.[17]
Complications
Complications of hemorrhage occur as a result of decreased blood flow to organs and, ultimately, tissue hypoxia; this can lead to organ failure, seizures, coma, and death. When the brain is deprived of oxygen for prolonged periods, it can result in tissue infarction that often leads to long-term neurological and cognitive dysfunction. In particular, subarachnoid hemorrhaging can lead to vasospasms in the blood vessels during the weeks following a bleed and result in a stroke.[7] Other generalized complications include re-bleeding and complications related to hospitalization, including deep venous thrombosis and infection.[18]
Deterrence and Patient Education
Following a hemorrhage, patients need education on what to expect in their recovery and how to avoid future recurrence. Studies have found that survivors often do not reach their rehabilitation goals and report a lack of accessibility to resources. Before discharge, patients should discuss with the healthcare team the goals for rehabilitation and how they can seek support during their recovery. Patients and their families also need education on what to expect in the recovery process. Providing access to social and financial support can help manage the stressors that arise.
Enhancing Healthcare Team Outcomes
Uncontrolled hemorrhage remains a leading cause of death and is potentially preventable. Patient outcomes are largely dependent on timely and appropriate interventions. Currently, there is no widely approved educational tool available to train healthcare personnel in the workplace. An interprofessional team that includes nurses is essential in the management of patients with hemorrhage. A recent study published in "The Forgotten Survivor" (Jones, 2006) showed that a hospital-wide basic learning module on recognizing hemorrhage was effective in helping healthcare workers feel more prepared to assist in hemorrhage management.[19]
Hemorrhage management requires an interprofessional team approach, including physicians, specialists, specialty-trained nurses, and pharmacists collaborating across disciplines to achieve optimal patient results. Nurses are required to assist with monitoring and educating families during a crisis and in hemorrhage control procedures. The pharmacist may need to work with the clinicians to make appropriate treatment choices if the cause of the bleeding is directly or indirectly medication-related. A team approach to dealing with acute hemorrhage will provide the best outcomes. [Level 5]
Media
(Click Image to Enlarge)
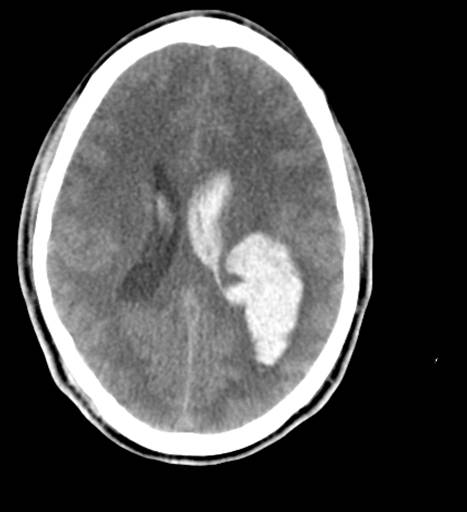
Head CT, Intraventricular and Intraparenchymal Hemorrhage From Arteriovenous Malformations (AVM)
Contributed by Scott Dulebohn, MD
(Click Image to Enlarge)
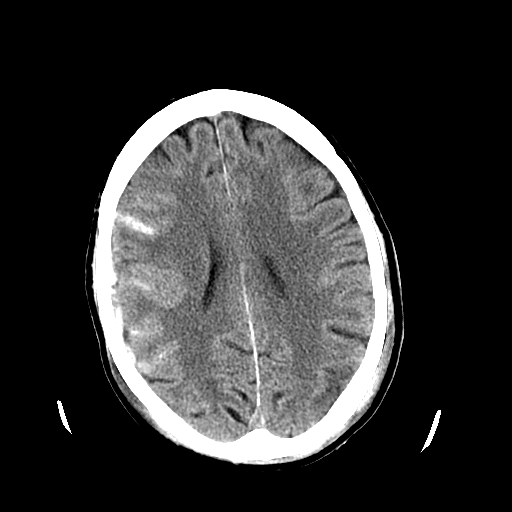
Head CT Revealing Subarachnoid Hemorrhage. The image depicts a head CT scan of a patient revealing a subarachnoid hemorrhage.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)

Splinter, Hemorrhage, Nail Anatomy, Finger Contributed by Steve Bhimji, MS, MD, PhD
(Click Image to Enlarge)

Retrobulbar Hematoma. The patient developed severe pain in the left eye and orbit after an uneventful upper blepharoplasty. The patient was not seen and examined until the following morning when this photograph was taken. The patient has no perception of light in the left eye. A canthotomy, cantholysis, and evacuation of orbital hemorrhage did not help this patient, as this should have been performed much earlier.
Contributed by Prof. BCK Patel MD, FRCS
(Click Video to Play)
References
Lee SU, Kim T, Kwon OK, Bang JS, Ban SP, Byoun HS, Oh CW. Trends in the Incidence and Treatment of Cerebrovascular Diseases in Korea : Part I. Intracranial Aneurysm, Intracerebral Hemorrhage, and Arteriovenous Malformation. Journal of Korean Neurosurgical Society. 2020 Jan:63(1):56-68. doi: 10.3340/jkns.2018.0179. Epub 2019 May 8 [PubMed PMID: 31064041]
Gross BA, Jankowitz BT, Friedlander RM. Cerebral Intraparenchymal Hemorrhage: A Review. JAMA. 2019 Apr 2:321(13):1295-1303. doi: 10.1001/jama.2019.2413. Epub [PubMed PMID: 30938800]
Agarwal S, Zhou T, Frontera J. Journal Club: Association between aspirin dose and subarachnoid hemorrhage from saccular aneurysms: A case-control study. Neurology. 2019 May 7:92(19):920-922. doi: 10.1212/WNL.0000000000007460. Epub [PubMed PMID: 31061211]
Level 2 (mid-level) evidencePontius E, Vieth JT. Complications in Early Pregnancy. Emergency medicine clinics of North America. 2019 May:37(2):219-237. doi: 10.1016/j.emc.2019.01.004. Epub [PubMed PMID: 30940368]
Baekgaard JS, Eskesen TG, Lee JM, Yeh DD, Kaafarani HMA, Fagenholz PJ, Avery L, Saillant N, King DR, Velmahos GC. Spontaneous Retroperitoneal and Rectus Sheath Hemorrhage-Management, Risk Factors and Outcomes. World journal of surgery. 2019 Aug:43(8):1890-1897. doi: 10.1007/s00268-019-04988-y. Epub [PubMed PMID: 30963204]
Lazarev A, Golokhvast K, Borozda I. Review of the Problems of Diagnosis of Endopelvic Haemorrhage, Its Intensity, Volume, and Duration, and Treatment Methods of Circulatory Injuries and Surgical Hemostasis after Pelvic Fractures. Emergency medicine international. 2019:2019():2514146. doi: 10.1155/2019/2514146. Epub 2019 Feb 19 [PubMed PMID: 30915239]
Matano F, Fujiki Y, Mizunari T, Koketsu K, Tamaki T, Murai Y, Yokota H, Morita A. Serum Glucose and Potassium Ratio as Risk Factors for Cerebral Vasospasm after Aneurysmal Subarachnoid Hemorrhage. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2019 Jul:28(7):1951-1957. doi: 10.1016/j.jstrokecerebrovasdis.2019.03.041. Epub 2019 May 3 [PubMed PMID: 31060790]
Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. The Journal of trauma. 2006 Jun:60(6 Suppl):S3-11 [PubMed PMID: 16763478]
Level 3 (low-level) evidenceCarmichael H, Steward L, Peltz ED, Wright FL, Velopulos CG. Preventable death and interpersonal violence in the United States: Who can be saved? The journal of trauma and acute care surgery. 2019 Jul:87(1):200-204. doi: 10.1097/TA.0000000000002336. Epub [PubMed PMID: 31045724]
Foucher CD, Tubben RE. Lactic Acidosis. StatPearls. 2024 Jan:(): [PubMed PMID: 29262026]
Mackenzie MJ, Hiranandani R, Wang D, Fung T, Lang E. Determinants of Computed Tomography Head Scan Ordering for Patients with Low-Risk Headache in the Emergency Department. Cureus. 2017 Oct 9:9(10):e1760. doi: 10.7759/cureus.1760. Epub 2017 Oct 9 [PubMed PMID: 29226050]
Kim du S, Kong MH, Jang SY, Kim JH, Kang DS, Song KY. The usefulness of brain magnetic resonance imaging with mild head injury and the negative findings of brain computed tomography. Journal of Korean Neurosurgical Society. 2013 Aug:54(2):100-6. doi: 10.3340/jkns.2013.54.2.100. Epub 2013 Aug 31 [PubMed PMID: 24175023]
Aboudara M, Maldonado F. Update in the Management of Pleural Effusions. The Medical clinics of North America. 2019 May:103(3):475-485. doi: 10.1016/j.mcna.2018.12.007. Epub [PubMed PMID: 30955515]
Nixon G, Blattner K, Muirhead J, Finnie W, Lawrenson R, Kerse N. Scope of point-of-care ultrasound practice in rural New Zealand. Journal of primary health care. 2018 Oct:10(3):224-236. doi: 10.1071/HC18031. Epub [PubMed PMID: 31039937]
Rubano E, Mehta N, Caputo W, Paladino L, Sinert R. Systematic review: emergency department bedside ultrasonography for diagnosing suspected abdominal aortic aneurysm. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2013 Feb:20(2):128-38. doi: 10.1111/acem.12080. Epub [PubMed PMID: 23406071]
Level 3 (low-level) evidenceVulliamy P, Thaventhiran AJ, Davenport RA. What's new for trauma haemorrhage management? British journal of hospital medicine (London, England : 2005). 2019 May 2:80(5):268-273. doi: 10.12968/hmed.2019.80.5.268. Epub [PubMed PMID: 31059346]
Palmer L. Fluid Management in Patients with Trauma: Restrictive Versus Liberal Approach. The Veterinary clinics of North America. Small animal practice. 2017 Mar:47(2):397-410. doi: 10.1016/j.cvsm.2016.10.014. Epub 2016 Dec 1 [PubMed PMID: 27914759]
Level 3 (low-level) evidenceDhakal P, Wang L, Gardiner J, Shrotriya S, Sharma M, Rayamajhi S. Effectiveness of Sequential Compression Devices in Prevention of Venous Thromboembolism in Medically Ill Hospitalized Patients: A Retrospective Cohort Study. Turkish journal of haematology : official journal of Turkish Society of Haematology. 2019 Aug 2:36(3):193-198. doi: 10.4274/tjh.galenos.2019.2018.0413. Epub 2019 May 1 [PubMed PMID: 31042860]
Level 2 (mid-level) evidenceHegvik JR, Spilman SK, Olson SD, Gilchrist CA, Sidwell RA. Effective Hospital-Wide Education in Hemorrhage Control. Journal of the American College of Surgeons. 2017 May:224(5):796-799.e1. doi: 10.1016/j.jamcollsurg.2017.01.049. Epub 2017 Mar 22 [PubMed PMID: 28342652]