 McArdle Disease (Glycogen Storage Disease Type 5)
McArdle Disease (Glycogen Storage Disease Type 5)
Introduction
McArdle disease, also known as glycogen storage disorder (GSD) type 5, is a rare inherited metabolic disorder primarily affecting skeletal muscles. This condition arises from a deficiency or complete lack of the enzyme muscle glycogen phosphorylase (myophosphorylase), essential for breaking down glycogen into glucose, the primary energy fuel for muscle cells. The disease follows an autosomal recessive inheritance pattern, meaning both gene copies must be mutated for the condition to manifest.[1]
In McArdle disease, the absence of myophosphorylase leads to the accumulation of glycogen in muscle tissues, as it cannot be adequately broken down to release glucose. Although glycolysis—the process of converting glucose to energy—is impaired, it is not completely blocked. Muscle fibers can still metabolize glucose to glucose-6-phosphate (G6P) downstream of the metabolic block, allowing partial energy production. This incomplete disruption leads to characteristic clinical symptoms, ranging from exercise intolerance, muscle cramps, and fatigue to more severe complications, eg, rhabdomyolysis, which is muscle breakdown during strenuous activities.[2]
Most patients with GSDs present in childhood; however, McArdle disease is one of those that have adult-onset forms as well. Unfortunately, treatment options are few and far between, although diet therapy has been observed to be efficacious in reducing clinical manifestations.
McArdle disease was first reported in 1951 by Dr. Brian McArdle from London. This was after a patient with myalgia failed to show increased blood lactate levels during exercise.[3] In 1959, it was described that the enzyme responsible for the affected step was myophosphorylase.[4][5] The underlying gene for myophosphorylase (PYGM) was first discovered in 1984.[6]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
McArdle disease typically results from mutations involving the muscle-specific isoform of the glycogen phosphorylase enzyme (abbreviated as PGYM). PGYM is also known as muscle glycogen phosphorylase (myophosphorylase, EC 2.4.1.1).[7] This enzyme plays a key role in the first step of glycogenolysis, which releases glucose-1-phosphate monomers in muscle fibers, releasing glucose from glycogenucose. As a result, the carbohydrate metabolism of the skeletal muscle is affected, and energy cannot be generated from the glycogen stores in muscles. The genetic mutations of the PYGM gene on 11q13 make the enzyme inactive.[8] Exons 1 and 17 are the areas with the most common mutations, with half of the identified mutations being missense variants. The commonest mutation in white individuals is described as p.Arg50Stop or R50X.[9][10]
As of 2015, 147 pathogenic mutations and 39 polymorphisms have been identified. The correlation between the genetic disorder and the associated phenotype is still not established despite the many mutations.[11] From the study of the genetics of McArdle disease, 179 variants have been identified that together affect the PYGM gene. Missense mutations are the most common variants in European and United States White populations (around 60% of all mutations). Studies have reported that most patients do not have myophosphorylase, regardless of the type of mutation, such as missense, nonsense, insertion, deletion, and splicing.[12] This indicates the absence of myophosphorylase activity when a PYGM mutation is present, except for those rare cases where missense mutations result in preserved myophosphorylase activity and better phenotypes.[13]
Epidemiology
The exact prevalence of McArdle disease is not precisely known and appears to range from 1 in 50,000 to 1 in 200,000 in the United States. The variation between the prevalence according to genetic data and the prevalence according to diagnosed cases is attributable to the delay in diagnosis. One study analyzed gene frequency and next-generation sequencing data to report the true prevalence of the disease among populations. The study's results revealed that the disease is much more common than previously thought and has a prevalence of 1 in 7,650 (95% confidence interval (CI) 1/5,362 to 1/11,108). An additional method used by the same study looked at the 2 most common mutations and recorded a prevalence of 1 in 42,355.[14][10]
In some areas of the United States, eg, the Dallas/Fort Worth area, the prevalence of McArdle disease based on genetic data is reported to be 1/100,000.[15] A study in 2015 in Spain reported the prevalence of diagnosed cases to be around 1/139,543, up from 2011, when the prevalence was estimated at 1/167,000.[16]
In terms of gender, in McArdle disease, the following ratios of men to women have been noted:
In terms of age, most McArdle disease cases present in the second or third decade of life. Wolfe et al report a unique precedent of McArdle disease manifesting in a 73-year-old patient.[19] Felice and Pourmand also reported late presentations. Clinicians should consider the diagnosis of McArdle disease regardless of the age of presentation.[20][21] Despite being a rare condition typically diagnosed after a prolonged period, improvements in diagnostic technology have led to a rise in identified cases. This indicates that many individuals likely remain undiagnosed due to past challenges in detection.
Pathophysiology
Myophosphorylase is a key enzyme in regulating glucose metabolism in muscles. It detaches 1,4 glycosyl chains from glycogen and attaches inorganic phosphate to form glucose-1-phosphate. During glycogen breakdown, muscle cells generate glucose-1-phosphate in place of glucose, and due to the former molecule's polar nature, it disintegrates intracellularly.
PYGM is activated when phosphorylated by the enzyme phosphorylase kinase. Glucagon and adrenaline initiate glycogenolysis in the liver, binding to G-protein coupled receptors first. The signaling pathway behind this process involves G-protein coupled receptors (GPCRs), adenylate cyclase (AC), cyclic adenosine monophosphate (cAMP), protein kinase A (PKA), and phosphorylase kinase (PK) causing PYGM activation. In contrast, PYGM becomes inactivated when dephosphorylated by a different enzyme called protein phosphatase 1 (PP1).[9]
Several tissue-specific isoforms of phosphorylase exist. Myophosphorylase is found in cardiac myocytes and the brain and is the only variant in skeletal muscle. Most patients with McArdle disease lack myophosphorylase activity; therefore, they are unable to produce energy in the form of glucose by breaking down glycogen stores in muscles.[22]
During aerobic activity, eg, walking, jogging, gentle swimming, or cycling, the skeletal muscle derives energy from free fatty acids by oxidizing them in the mitochondria via the beta-oxidation pathway to form acetyl-CoA. Acetyl-CoA is further metabolized via the Krebs cycle and the respiratory chain, producing adenosine triphosphate (ATP). During anaerobic activity, such as weightlifting or sprinting, the myophosphorylase of the skeletal muscle breaks down glycogen to glucose, which then enters the glycolytic pathway, yielding ATP anaerobically.[23]
Myophosphorylases are vital enzymes in muscle glucose metabolism, breaking down glycogen into glucose-1-phosphate. Myophosphorylases are activated by phosphorylase kinase through a hormone-triggered signaling cascade involving glucagon and adrenaline, while it is deactivated by protein phosphatase 1. Myophosphorylase is present in skeletal muscle, cardiac muscle, and the brain, but its absence in skeletal muscle, as seen in McArdle disease, impairs the muscle's ability to produce energy from glycogen. During aerobic exercise, muscles rely on fat oxidation for energy, while anaerobic activities use glycogen breakdown through the glycolytic pathway to generate ATP.
Histopathology
Muscle tissue is biopsied and examined under a microscope to support the diagnosis. The hallmark findings suggestive of McArdle disease are glycogen deposits and the absence of the enzyme myophosphorylase.[24] Glycogen deposits appear under the sarcolemmal membrane at the periphery of myofibers. The collection of glycogen between myofibrils makes the myofibers look like vacuoles (see Image. Histopathology of McArdle Disease). The glycogen takes up periodic acid-Schiff. The absence of glycogen accumulation in muscle biopsy should not be taken as proof for the absence of McArdle disease, as the glycogen could be washed out in tissue processing.
Myophosphorylase histochemistry is easier to perform and has a good negative predictive value. Its absence is diagnostic for McArdle disease. However, clinicians must specifically request the testing of myophosphorylase. Given that the accumulation of subsarcolemmal glycogen has been recognized as a key histological diagnostic marker for McArdle disease, reduced or absent myophosphorylase enzyme activity in muscle biopsy serves as a histochemical diagnostic feature. In a study of 60 patients in 2020, the histological and histochemical findings in this patient population, showing sub-sarcolemmal glycogen buildup and a lack of myophosphorylase activity in muscle biopsies, further support these diagnostic criteria.[25]
History and Physical
Clinical Symptoms
The most frequently reported symptom of McArdle disease is physical activity intolerance. Other symptoms include painful muscle cramps, weakness, and fatigue. Muscle pain and stiffness can sometimes lead to painful contractures. All these symptoms are much more pronounced soon after starting activity and are alleviated with exercise cessation.
During episodes of sudden, prolonged muscle contraction during high-intensity exercise, severe muscle damage can occur, releasing muscle proteins like creatine kinase (often exceeding 1,000 U/L) and myoglobin into the bloodstream. This can also cause myoglobinuria, which is characterized by dark-colored urine. In rare cases, such an episode of rhabdomyolysis and muscle breakdown may result in acute renal failure and life-threatening hyperkalemia.[26]
In a study of 60 patients in 2020, 100% of the patients reported experiencing exercise-induced muscle pain, and nearly half had persistent muscle weakness. Although most patients had symptom onset before age 15, the average age at diagnosis was 37 years old. A positive family history of McArdle disease was noted in 25% of cases, and more than half reported experiencing the "second-wind" phenomenon when asked.[25] This unique feature of the second-wind phenomenon is seen in most patients of McArdle disease and is characterized by improved symptoms after approximately 10 minutes of gentle aerobic activity.[10]
McArdle disease usually presents in the first or second decade of life. Patients older than 40 years complain of weakness and wasting of muscles.[27][28][10][9][24] Clinical heterogeneity is widely seen in this disease. Some patients present with very mild symptoms, such as tiredness without cramps. On the other hand, progressive weakness ensues in the 6th or 7th decade of life. Contrary to this, fatal infantile McArdle syndrome, which is the severe and rapidly progressive form, appears shortly after birth. Seizures have been described in 4% of affected patients.
Physical Examination Findings
Classic McArdle disease presents with the following examination findings:
- Proximal muscle weakness, most notable following exercise
- Fixed limb weakness, usually in the proximal muscle groups
- Muscle wasting
The fatal infantile variant can have the following examination findings:
- Hypotonia
- Diminished deep tendon reflexes
Evaluation
Exercise Testing
A forearm exercise test is used for initial assessment in suspected cases of McArdle disease. Because glycogenolysis is defective, no pyruvate and subsequent lactate are produced through normal pathways. Isometric rhythmic exercises are performed for 1 minute, and the lactate and ammonia levels are compared before and after the exercise. A 3-fold rise in lactate and ammonia occurs during normal circumstances, but the lactate rise is remarkably low in glycolytic and glycogenolytic disorders.
The ischemic test using a sphygmomanometer cuff is obsolete now, and a recent consensus on using nonischemic forearm exercise tests was established to avoid unfavorable outcomes like rhabdomyolysis and compartment syndrome.[29] The test has fairly high sensitivity and specificity; therefore, a normal test result rules out the possibility of a glycolytic or glycogenolytic defect. Nonischemic forearm testing is equally diagnostic, with a lesser risk of compartment syndrome. These tests are performed similarly but without a blood pressure cuff.[30] The nonischemic test has a sensitivity of 100% and a specificity of 100% and 99.7%, respectively, as reported by a 2015 retrospective study.[31]
A characteristic feature of McArdle disease is the chronically elevated serum creatine kinase (CK) enzyme levels. In a study of 60 patients in 2020, serum creatine kinase levels were elevated 5 to 18 times above the upper reference limit in 100% of patients assessed. In the forearm ischemic lactate test, the change in lactate levels among the affected patients was significantly lower than in controls. Conversely, the change in ammonia levels in patients was significantly higher than in controls. The myophosphorylase enzyme activity in muscle homogenates was markedly reduced in all 20 patients whose muscle samples were analyzed. 60% of affected patients showed a complete absence of enzyme activity.[10]
Graded exercise stress demonstrates the second-wind phenomenon often seen in patients with McArdle disease and helps distinguish it from disorders of glycolytic pathways.
Additional Diagnostic Evaluation
Muscle biopsy (vastus lateralis or biceps brachialis) shows periodic acid Schiff-positive vacuoles of high glycogen content and absence of myophosphorylase. Genetic testing includes options of specific mutation analysis (most commonly R50X in white population), next-generation PYGM gene sequencing panels, myopathy panels, or whole-exome sequencing for particular glycogen-storage diseases. Typically, patients are diagnosed based on whether they are homozygous or compound heterozygous for PYGM pathogenic mutations. A study aimed to formulate a less invasive approach to diagnose the disease and determine PYGM expression in white blood cells using antibodies.
A study in 2022 analyzed whole-body magnetic resonance imaging (WB-MRI) scans of 15 genetically confirmed McArdle disease patients and highlighted muscle involvement at different disease stages. Fatty substitution was assessed in 60 muscles, with common findings of mild fixed muscle weakness, particularly in the neck flexors and proximal muscles, and moderate scapular winging in some cases. WB-MRI revealed recurrent muscle changes in specific muscles and proved to be a valuable diagnostic tool for McArdle disease. Thus, MRI in affected areas could be a useful adjunct in diagnosing this condition.[32]
Other tests performed to support the findings are serum uric acid levels (high in about half of the cases), urinalysis for detecting pigmenturia, and electromyography, which often yields normal findings.[10][33][30][8][24]
Evaluation in Children
Based on the most recent guidelines, diagnosing GSD type 5 in young children is challenging. The second-wind phenomenon, where patients experience a sudden boost in physical stamina, may not be easy to detect in children. Diagnosing GSD often involves complex tests, including genetic screening and nonischemic forearm exercise tests, although these tests are hard to perform in young children. Misdiagnosis is common, with 90% of GSD type 5 patients receiving an incorrect diagnosis initially, leading to delayed treatment and potential complications such as rhabdomyolysis or acute renal failure. Genetic testing plays a critical role in diagnosis, with over 179 variants of GSD type 5 identified. Muscle biopsies may be used when other diagnostic tools are inconclusive. Accurate diagnosis is vital to improving long-term management.[34]
Treatment / Management
Modified Activity Therapies
The treatment focuses mainly on avoiding lifestyle activities that exacerbate the symptoms. Patients may adapt to avoiding physical activity, which may worsen the disease because serum CK rises with loss of aerobic fitness. Avoiding activity may also decrease the capacity of muscles to utilize alternate fuels to overcome the block in glycogenolysis. Moreover, a marked reduction in the expression of proteins needed for metabolism and calcium hemostasis occurs in nonexercising muscles.
Studies have documented the beneficial effects of moderate-intensity graded aerobic exercise therapy. With this intervention, patients reported less significant exercise intolerance and an earlier appearance of a second wind. A balanced weight-lifting approach also lessened the severity of symptoms in some patients.
Medical Therapies
Howell et al proposed that sodium valproate could cause the up-regulation of the myophosphorylase enzyme. The findings of that study suggested that sodium valproate could be a potential management option for McArdle disease; however, more randomized trials are needed.[35](B3)
Creatine may improve ATP storage and exercise tolerability. However, in a trial, high-dose creatine monohydrate resulted in poor exercise tolerance and increased exercise-induced myalgia significantly. The investigators proposed an explanation that inadequate adaptation to better electromechanical efficacy results in excess muscle contractility during exercise and, thus, a resultant worsening of symptoms.[36](A1)
Dietary Modification
Certain dietary interventions that confer favorable effects include taking a sugary meal before planned exercise—for example, having a drink containing 37 g sucrose 5 minutes before exercise reduces initial symptoms of exercise intolerance. A carbohydrate-rich diet results in much better outcomes than a protein-rich diet. Other nutritional agents that were helpful for some patients but could not yield convincing outcomes during actual experimental studies include branched-chain amino acids, depot glucagon preparations, verapamil, dantrolene sodium, vitamin B6, high dose D-ribose, and high-dose creatine ingestion.[37][28][26][38][10][39](A1)
Ongoing Research
A study on the EUROMAC registry in 2023 enhances understanding of GSD type 5 and encourages clinicians to create registries for other rare diseases. This paper’s analyses provide insight into the functional limitations, treatments, and rehabilitation strategies for GSD type 5. The findings align with recent international recommendations, advocating for an active, healthy lifestyle and cautious use of analgesics. Additionally, participants reported positive effects from diet and supplementation.[40]
A new medication was studied, called Mavoldepar a peroxisome proliferator-activated receptor delta (PPARδ) agonist that would ehance the quality of life for patients with McArdle disease. However, the phase 3 clinical trial did not show promising results and was stopped for failing to meet its outcomes. The search for a medication that would help patients with Mcardle continues. https://clinicaltrials.gov/study/NCT04535609
Differential Diagnosis
Distinguishing McArdle disease from other glycogen storage disorders, as well as other diseases inducing myopathy, is critical, particularly fatty acid oxidation defects and mitochondrial myopathies.
McArdle disease manifests its symptoms at the very beginning of rigorous physical activity, whereas fatty acid oxidation defects (carnitine palmitoyltransferase II deficiency) and mitochondrial myopathies (medium-chain acyl-CoA dehydrogenase deficiency) show symptoms much later and during a longer duration of exercise. Moreover, fatty acid oxidation defects manifest symptoms during stressful states such as fasting, fever, and infections.
A noteworthy phenomenon associated with McArdle disease is the second wind phenomenon (lesser perception of discomfort), which does not occur in other conditions with similar clinical features. Patients with McArdle disease have chronically high serum creatine kinase levels. This enzyme may or may not be elevated in other glycogen storage diseases, fatty acid oxidation defects, and mitochondrial myopathies.
Given that McArdle disease presents with exercise intolerance, muscle pain, cramps, and myoglobinuria, the differential diagnoses include other glycogen storage diseases like Cori (GSD type 3) and Tarui disease (GSD type 7), mitochondrial myopathies, and inflammatory myopathies like polymyositis. Rhabdomyolysis, muscular dystrophies, and periodic paralysis syndromes should also be considered. Key distinguishing features include the second-wind phenomenon and lack of lactate elevation during exercise testing in McArdle disease.[41]
Generally, a carbohydrate-rich meal before exercise decreases the severity of symptoms in McArdle disease and fatty acid oxidation defects. However, it is not proven to be helpful in mitochondrial myopathies, as it worsens symptoms in the glycolytic pathway disorder.
Muscle biopsy and genetic testing further delineate the differences between differential diagnoses. McArdle disease on biopsy shows high glycogen content, carnitine palmitoyltransferase II deficiency shows increased lipids, mitochondrial myopathy shows ragged red fibers, and cytochrome oxidase negative fibers. Specific mutation analysis reveals that the most common mutations are R50X, S113L, and m.3243A>G in McArdle disease, fatty acid oxidation disorders, and mitochondrial defects.[24]
Prognosis
Most patients affected with McArdle disease lead a normal life, and it does not affect life expectancy. Rhabdomyolysis is to be avoided as it can lead to acute renal failure, which may potentially become life-threatening. Patients exploit the second wind phenomenon and adjust to the disease itself. Only a minority of patients have been known to experience progressive worsening of symptoms with advancing age and wasting, especially over the shoulder girdle and back muscles.[28]
More recent studies report heterogeneity in the clinical severity, such as 8% of patients being asymptomatic in daily life and 21% showing limitations in the activities of daily living and fixed muscle weakness.[16] The evidence also reiterates acquiring an active lifestyle, which is critical in patients with McArdle disease.[16]
In the study on the EUROMAC registry in 2023, two-thirds of participants worked, with the highest employment rates among those aged 20 to 60. Around 29% reported changing jobs due to GSD type 5, and 22% required workplace accommodations for their condition. Over half of the participants described their work as primarily sedentary, one-third mainly walked, and 13% had physically demanding jobs. The remaining third were not employed at the time of the study, emphasizing the need for future options to improve the quality of life.[40] Various studies have also reported that the disease does not adversely alter the course of pregnancy or childbirth.[26]
Complications
Rhabdomyolysis is an established complication of McArdle disease.[42] Acute renal failure may result from myoglobinuria after vigorous exercise. As with any patient having rhabdomyolysis, patients with McArdle disease should be monitored for the possible complications of electrolyte abnormalities, hyperuricemia, compartment syndrome, and metabolic encephalopathy.[43] Based on the most recent clinical practice guidelines, individuals with GSD type 5 or GSD type 7 are at risk of rhabdomyolysis with all the subsequent associated complications.[34]
Deterrence and Patient Education
Upon diagnosis of the condition, clinicians should refer the patient to a clinical geneticist or genetic counselor. Annual surveillance includes routine physical examinations and diet checks. Counseling consists of avoiding certain exercises, eg, sustained hand grip exercises, weight lifting unless under a specialist's supervision, competitive ball games, running, exercises involving excessive jumping, strenuous swimming, and cycling.[27][16][10][28] Limitation or adaptation of physical activity to avoid symptoms is necessary, as rhabdomyolysis is a life-threatening condition. A mild risk of acute muscle necrosis is present secondary to certain general anesthetics, eg, muscle relaxants and inhaled anesthetic agents.[44]
For patients with GSD type 5, diagnosis and management should be led by a clinical team at a Center of Excellence (CoE). Regular monitoring of CK levels is essential, as CK elevation may indicate muscle breakdown rather than cardiac issues. Anesthetic procedures require special precautions to avoid triggering muscle contractures or rhabdomyolysis. Medication interactions must also be carefully considered, with an emphasis on avoiding statins and systemic steroids that may worsen muscle symptoms. Additionally, obstetric care requires caution to minimize muscle fatigue and cramps in pregnant women with GSD, though most can have normal deliveries.
Blood pressure cuffs should be removed quickly during examinations in patients with GSD type 5 or GSD type 7 to avoid damaging muscle tissue due to restricted blood flow. Static muscle positions and compression should also be minimized to prevent cramps or contractures. Massage and chiropractic treatments can help relieve chronic pain, but therapists must be cautious and avoid placing undue stress on muscles to prevent further injury. Patients should carry an emergency card or use an "In Case of Emergency" app to recognize symptoms, including myoglobinuria, severe muscle pain, weakness, and swelling, and seek immediate medical attention if these symptoms present. They should stay well hydrated while waiting for further medical treatment.[34]
Enhancing Healthcare Team Outcomes
Managing McArdle disease (GSD type 5) requires a comprehensive, patient-centered approach involving an interprofessional team to optimize care, enhance outcomes, and ensure patient safety. Physicians, advanced practitioners, nurses, pharmacists, genetic specialists, therapists, and anesthetists must collaborate effectively to address the complex needs of individuals with this autosomal recessive disorder. Patients and their families benefit from genetic counseling to understand the inheritance pattern and potential risks for future generations. Genetic testing may be offered to relatives, particularly siblings, as carriers often remain asymptomatic but can transmit the condition. Family planning discussions should include options such as prenatal and preimplantation genetic testing, empowering patients to make informed decisions.
Interprofessional care coordination plays a pivotal role in improving patient outcomes. Clinicians provide education on symptom recognition, safe exercise practices, and emergency preparedness, helping patients navigate their condition while minimizing risks. Specialists monitor disease progression and tailor management plans, while therapists deliver gentle interventions to alleviate chronic pain and prevent exacerbations. Anesthetists adhere to strict protocols during surgical procedures to prevent muscle damage, ensuring patient safety in these high-risk scenarios. Obstetric care may involve customized exercise regimens and strategies to reduce muscle contracture risks during and after pregnancy.
Frequent communication, shared decision-making, and coordinated efforts among healthcare professionals ensure that each patient’s care is holistic and individualized. This collaborative model enhances team performance, prioritizes patient safety, and improves the overall quality of life for individuals with McArdle disease.
Media
(Click Image to Enlarge)

Histopathology of McArdle Disease. This image shows vacuoles in myocytes, a pathological characteristic of McArdle disease.
Jensflorian, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
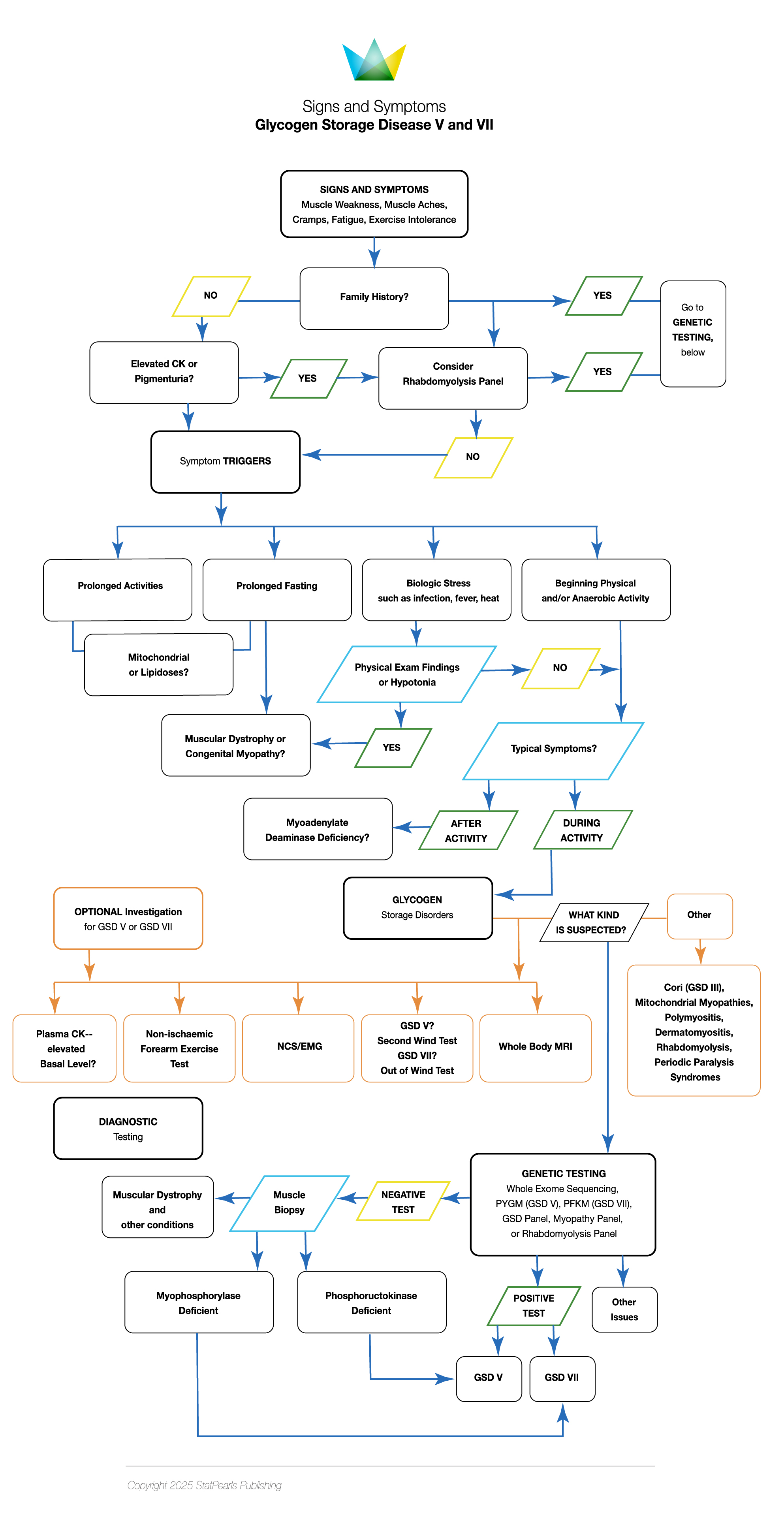
Glycogen Storage Disease V and VII, Signs and Symptoms.
Illustration by K Humphreys
(Click Image to Enlarge)
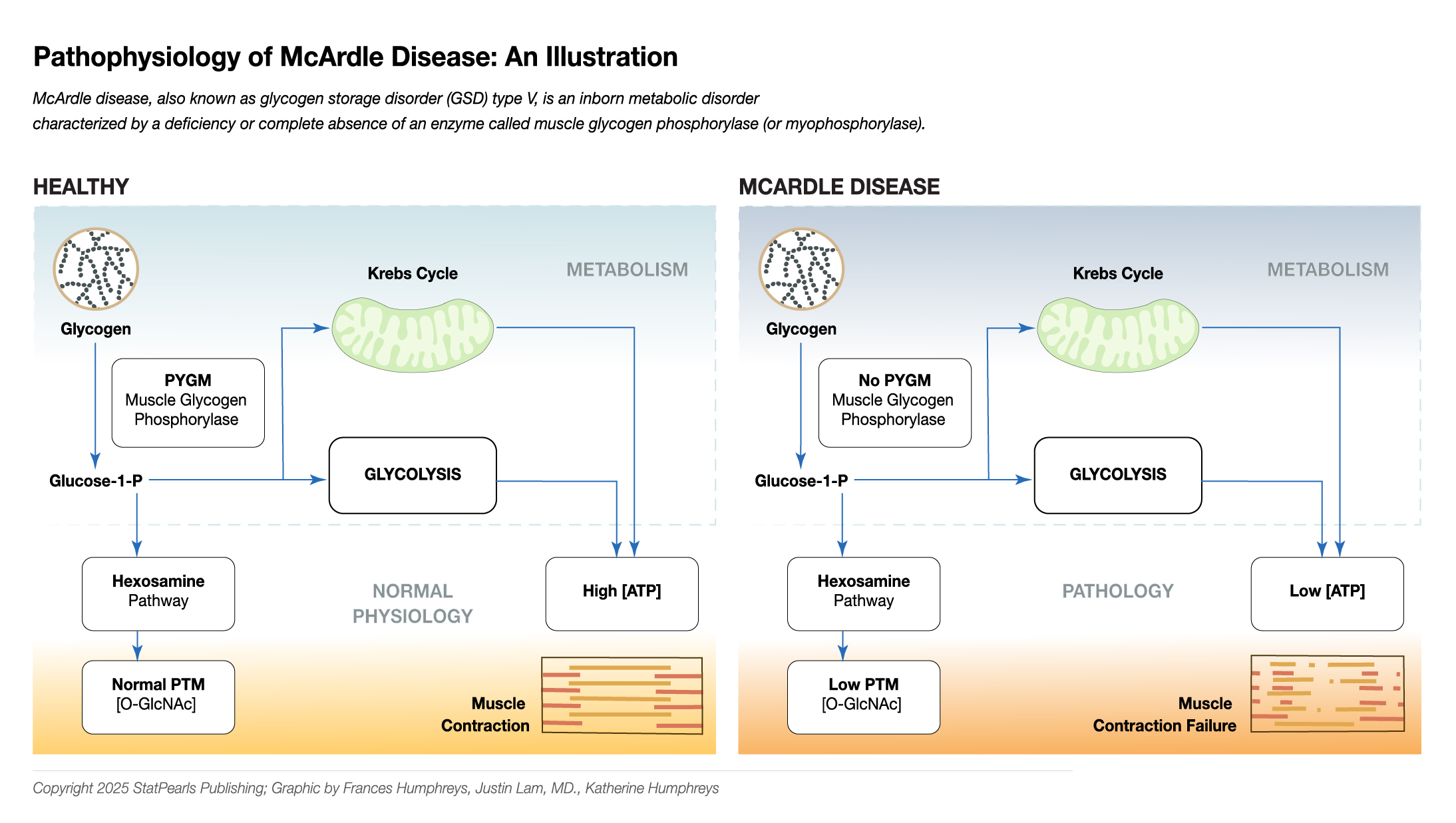
Pathophysiology of McArdle Disease.
Illustrated and contributed by F Humphreys, J Lam, MD, and K Humphreys
References
Santalla A, Nogales-Gadea G, Ørtenblad N, Brull A, de Luna N, Pinós T, Lucia A. McArdle disease: a unique study model in sports medicine. Sports medicine (Auckland, N.Z.). 2014 Nov:44(11):1531-44. doi: 10.1007/s40279-014-0223-5. Epub [PubMed PMID: 25028051]
Level 3 (low-level) evidenceFukui T, Shimomura S, Nakano K. Potato and rabbit muscle phosphorylases: comparative studies on the structure, function and regulation of regulatory and nonregulatory enzymes. Molecular and cellular biochemistry. 1982 Feb 19:42(3):129-44 [PubMed PMID: 7062910]
Level 2 (mid-level) evidenceMcARDLE B. Myopathy due to a defect in muscle glycogen breakdown. Clinical science. 1951 Feb:10(1):13-35 [PubMed PMID: 24540673]
Mommaerts WF, Illingworth B, Pearson CM, Guillory RJ, Seraydarian K. A FUNCTIONAL DISORDER OF MUSCLE ASSOCIATED WITH THE ABSENCE OF PHOSPHORYLASE. Proceedings of the National Academy of Sciences of the United States of America. 1959 Jun:45(6):791-7 [PubMed PMID: 16590445]
SCHMID R, MAHLER R. Chronic progressive myopathy with myoglobinuria: demonstration of a glycogenolytic defect in the muscle. The Journal of clinical investigation. 1959 Nov:38(11):2044-58 [PubMed PMID: 14442994]
Lebo RV, Gorin F, Fletterick RJ, Kao FT, Cheung MC, Bruce BD, Kan YW. High-resolution chromosome sorting and DNA spot-blot analysis assign McArdle's syndrome to chromosome 11. Science (New York, N.Y.). 1984 Jul 6:225(4657):57-9 [PubMed PMID: 6587566]
Level 3 (low-level) evidenceAndreu AL, Nogales-Gadea G, Cassandrini D, Arenas J, Bruno C. McArdle disease: molecular genetic update. Acta myologica : myopathies and cardiomyopathies : official journal of the Mediterranean Society of Myology. 2007 Jul:26(1):53-7 [PubMed PMID: 17915571]
de Luna N, Brull A, Lucia A, Santalla A, Garatachea N, Martí R, Andreu AL, Pinós T. PYGM expression analysis in white blood cells: a complementary tool for diagnosing McArdle disease? Neuromuscular disorders : NMD. 2014 Dec:24(12):1079-86. doi: 10.1016/j.nmd.2014.08.002. Epub 2014 Aug 21 [PubMed PMID: 25240406]
Level 2 (mid-level) evidenceLlavero F, Arrazola Sastre A, Luque Montoro M, Gálvez P, Lacerda HM, Parada LA, Zugaza JL. McArdle Disease: New Insights into Its Underlying Molecular Mechanisms. International journal of molecular sciences. 2019 Nov 25:20(23):. doi: 10.3390/ijms20235919. Epub 2019 Nov 25 [PubMed PMID: 31775340]
Nogales-Gadea G, Godfrey R, Santalla A, Coll-Cantí J, Pintos-Morell G, Pinós T, Arenas J, Martín MA, Lucia A. Genes and exercise intolerance: insights from McArdle disease. Physiological genomics. 2016 Feb:48(2):93-100. doi: 10.1152/physiolgenomics.00076.2015. Epub 2015 Oct 13 [PubMed PMID: 26465709]
Nogales-Gadea G,Brull A,Santalla A,Andreu AL,Arenas J,Martín MA,Lucia A,de Luna N,Pinós T, McArdle Disease: Update of Reported Mutations and Polymorphisms in the PYGM Gene. Human mutation. 2015 Jul; [PubMed PMID: 25914343]
García-Consuegra I, Asensio-Peña S, Ballester-Lopez A, Francisco-Velilla R, Pinos T, Pintos-Morell G, Coll-Cantí J, González-Quintana A, Andreu AL, Arenas J, Lucia A, Nogales-Gadea G, Martín MA. Missense mutations have unexpected consequences: The McArdle disease paradigm. Human mutation. 2018 Oct:39(10):1338-1343. doi: 10.1002/humu.23591. Epub 2018 Jul 26 [PubMed PMID: 30011114]
Vissing J, Duno M, Schwartz M, Haller RG. Splice mutations preserve myophosphorylase activity that ameliorates the phenotype in McArdle disease. Brain : a journal of neurology. 2009 Jun:132(Pt 6):1545-52. doi: 10.1093/brain/awp065. Epub 2009 May 11 [PubMed PMID: 19433441]
De Castro M, Johnston J, Biesecker L. Determining the prevalence of McArdle disease from gene frequency by analysis of next-generation sequencing data. Genetics in medicine : official journal of the American College of Medical Genetics. 2015 Dec:17(12):1002-6. doi: 10.1038/gim.2015.9. Epub 2015 Mar 5 [PubMed PMID: 25741863]
Haller RG. Treatment of McArdle disease. Archives of neurology. 2000 Jul:57(7):923-4 [PubMed PMID: 10891971]
Santalla A, Nogales-Gadea G, Encinar AB, Vieitez I, González-Quintana A, Serrano-Lorenzo P, Consuegra IG, Asensio S, Ballester-Lopez A, Pintos-Morell G, Coll-Cantí J, Pareja-Galeano H, Díez-Bermejo J, Pérez M, Andreu AL, Pinós T, Arenas J, Martín MA, Lucia A. Genotypic and phenotypic features of all Spanish patients with McArdle disease: a 2016 update. BMC genomics. 2017 Nov 14:18(Suppl 8):819. doi: 10.1186/s12864-017-4188-2. Epub 2017 Nov 14 [PubMed PMID: 29143597]
Bruno C, Cassandrini D, Martinuzzi A, Toscano A, Moggio M, Morandi L, Servidei S, Mongini T, Angelini C, Musumeci O, Comi GP, Lamperti C, Filosto M, Zara F, Minetti C. McArdle disease: the mutation spectrum of PYGM in a large Italian cohort. Human mutation. 2006 Jul:27(7):718 [PubMed PMID: 16786513]
Level 2 (mid-level) evidenceQuinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, Vissing J, Bruno C, Cassandrini D, Roberts M, Winer J, Rose M, Sewry C. McArdle disease: a clinical review. Journal of neurology, neurosurgery, and psychiatry. 2010 Nov:81(11):1182-8. doi: 10.1136/jnnp.2009.195040. Epub 2010 Sep 22 [PubMed PMID: 20861058]
Wolfe GI, Baker NS, Haller RG, Burns DK, Barohn RJ. McArdle's disease presenting with asymmetric, late-onset arm weakness. Muscle & nerve. 2000 Apr:23(4):641-5 [PubMed PMID: 10716777]
Level 3 (low-level) evidenceFelice KJ, Schneebaum AB, Jones HR Jr. McArdle's disease with late-onset symptoms: case report and review of the literature. Journal of neurology, neurosurgery, and psychiatry. 1992 May:55(5):407-8 [PubMed PMID: 1602316]
Level 3 (low-level) evidencePourmand R, Sanders DB, Corwin HM. Late-onset Mcardle's disease with unusual electromyographic findings. Archives of neurology. 1983 Jun:40(6):374-7 [PubMed PMID: 6573876]
Level 3 (low-level) evidenceDimaur S, Andreu AL, Bruno C, Hadjigeorgiou GM. Myophosphorylase deficiency (glycogenosis type V; McArdle disease). Current molecular medicine. 2002 Mar:2(2):189-96 [PubMed PMID: 11949935]
Level 3 (low-level) evidenceGodfrey R, Quinlivan R. Skeletal muscle disorders of glycogenolysis and glycolysis. Nature reviews. Neurology. 2016 Jul:12(7):393-402. doi: 10.1038/nrneurol.2016.75. Epub 2016 May 27 [PubMed PMID: 27231184]
Tarnopolsky MA. Metabolic Myopathies. Continuum (Minneapolis, Minn.). 2016 Dec:22(6, Muscle and Neuromuscular Junction Disorders):1829-1851 [PubMed PMID: 27922496]
Joshi PR, Deschauer M, Zierz S. McArdle Disease: Clinical, Biochemical, Histological and Molecular Genetic Analysis of 60 Patients. Biomedicines. 2020 Feb 15:8(2):. doi: 10.3390/biomedicines8020033. Epub 2020 Feb 15 [PubMed PMID: 32075227]
Lucia A, Ruiz JR, Santalla A, Nogales-Gadea G, Rubio JC, García-Consuegra I, Cabello A, Pérez M, Teijeira S, Vieitez I, Navarro C, Arenas J, Martin MA, Andreu AL. Genotypic and phenotypic features of McArdle disease: insights from the Spanish national registry. Journal of neurology, neurosurgery, and psychiatry. 2012 Mar:83(3):322-8. doi: 10.1136/jnnp-2011-301593. Epub 2012 Jan 16 [PubMed PMID: 22250184]
Level 2 (mid-level) evidenceAdam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, Martín MA, Lucia A, Arenas J, Andreu AL. Glycogen Storage Disease Type V. GeneReviews(®). 1993:(): [PubMed PMID: 20301518]
Quinlivan R, Martinuzzi A, Schoser B. Pharmacological and nutritional treatment for McArdle disease (Glycogen Storage Disease type V). The Cochrane database of systematic reviews. 2014 Nov 12:2014(11):CD003458. doi: 10.1002/14651858.CD003458.pub5. Epub 2014 Nov 12 [PubMed PMID: 25391139]
Level 1 (high-level) evidenceLucia A, Nogales-Gadea G, Pérez M, Martín MA, Andreu AL, Arenas J. McArdle disease: what do neurologists need to know? Nature clinical practice. Neurology. 2008 Oct:4(10):568-77. doi: 10.1038/ncpneuro0913. Epub [PubMed PMID: 18833216]
Kazemi-Esfarjani P, Skomorowska E, Jensen TD, Haller RG, Vissing J. A nonischemic forearm exercise test for McArdle disease. Annals of neurology. 2002 Aug:52(2):153-9 [PubMed PMID: 12210784]
Level 1 (high-level) evidenceHogrel JY, van den Bogaart F, Ledoux I, Ollivier G, Petit F, Koujah N, Béhin A, Stojkovic T, Eymard B, Voermans N, Laforêt P. Diagnostic power of the non-ischaemic forearm exercise test in detecting glycogenosis type V. European journal of neurology. 2015 Jun:22(6):933-40. doi: 10.1111/ene.12685. Epub 2015 Mar 5 [PubMed PMID: 25740218]
Level 2 (mid-level) evidenceTobaly D, Laforêt P, Stojkovic T, Behin A, Petit FM, Barp A, Bello L, Carlier P, Carlier RY. Whole-body muscle MRI in McArdle disease. Neuromuscular disorders : NMD. 2022 Jan:32(1):5-14. doi: 10.1016/j.nmd.2021.07.397. Epub 2021 Aug 5 [PubMed PMID: 34711478]
Hanisch F, Eger K, Bork S, Lehnich H, Deschauer M, Zierz S. Lactate production upon short-term non-ischemic forearm exercise in mitochondrial disorders and other myopathies. Journal of neurology. 2006 Jun:253(6):735-40 [PubMed PMID: 16619130]
Lucia A, Martinuzzi A, Nogales-Gadea G, Quinlivan R, Reason S, International Association for Muscle Glycogen Storage Disease study group. Clinical practice guidelines for glycogen storage disease V & VII (McArdle disease and Tarui disease) from an international study group. Neuromuscular disorders : NMD. 2021 Dec:31(12):1296-1310. doi: 10.1016/j.nmd.2021.10.006. Epub 2021 Oct 28 [PubMed PMID: 34848128]
Level 1 (high-level) evidenceHowell JM, Dunton E, Creed KE, Quinlivan R, Sewry C. Investigating sodium valproate as a treatment for McArdle disease in sheep. Neuromuscular disorders : NMD. 2015 Feb:25(2):111-9. doi: 10.1016/j.nmd.2014.10.002. Epub 2014 Oct 13 [PubMed PMID: 25455802]
Level 3 (low-level) evidenceVorgerd M, Zange J, Kley R, Grehl T, Hüsing A, Jäger M, Müller K, Schröder R, Mortier W, Fabian K, Malin JP, Luttmann A. Effect of high-dose creatine therapy on symptoms of exercise intolerance in McArdle disease: double-blind, placebo-controlled crossover study. Archives of neurology. 2002 Jan:59(1):97-101 [PubMed PMID: 11790236]
Level 1 (high-level) evidenceAndersen ST, Vissing J. Carbohydrate- and protein-rich diets in McArdle disease: effects on exercise capacity. Journal of neurology, neurosurgery, and psychiatry. 2008 Dec:79(12):1359-63. doi: 10.1136/adc.2008.146548. Epub [PubMed PMID: 19010947]
Level 1 (high-level) evidenceNogales-Gadea G, Consuegra-García I, Rubio JC, Arenas J, Cuadros M, Camara Y, Torres-Torronteras J, Fiuza-Luces C, Lucia A, Martín MA, García-Arumí E, Andreu AL. A transcriptomic approach to search for novel phenotypic regulators in McArdle disease. PloS one. 2012:7(2):e31718. doi: 10.1371/journal.pone.0031718. Epub 2012 Feb 9 [PubMed PMID: 22347505]
Level 2 (mid-level) evidenceSantalla A, Munguía-Izquierdo D, Brea-Alejo L, Pagola-Aldazábal I, Díez-Bermejo J, Fleck SJ, Ara I, Lucia A. Feasibility of resistance training in adult McArdle patients: clinical outcomes and muscle strength and mass benefits. Frontiers in aging neuroscience. 2014:6():334. doi: 10.3389/fnagi.2014.00334. Epub 2014 Dec 11 [PubMed PMID: 25566067]
Level 2 (mid-level) evidenceKarazi W, Scalco RS, Stemmerik MG, Løkken N, Lucia A, Santalla A, Martinuzzi A, Vavla M, Reni G, Toscano A, Musumeci O, Kouwenberg CV, Laforêt P, Millán BS, Vieitez I, Siciliano G, Kühnle E, Trost R, Sacconi S, Durmus H, Kierdaszuk B, Wakelin A, Andreu AL, Pinós T, Marti R, Quinlivan R, Vissing J, Voermans NC, EUROMAC Consortium. Data from the European registry for patients with McArdle disease (EUROMAC): functional status and social participation. Orphanet journal of rare diseases. 2023 Jul 25:18(1):210. doi: 10.1186/s13023-023-02825-z. Epub 2023 Jul 25 [PubMed PMID: 37488619]
Nascimento J,Pinho R,Pimenta de Castro A,Bernardino Vieira N, McArdle [PubMed PMID: 39318660]
Satoh A, Hirashio S, Arima T, Yamada Y, Irifuku T, Ishibashi H, Motoda A, Sueda Y, Masaki T. Novel Asp511Thr mutation in McArdle disease with acute kidney injury caused by rhabdomyolysis. CEN case reports. 2019 Aug:8(3):194-199. doi: 10.1007/s13730-019-00392-6. Epub 2019 Mar 21 [PubMed PMID: 30900170]
Level 3 (low-level) evidenceMull AB, Wagner JI, Myckatyn TM, Kells AF. Recurrent Compartment Syndrome Leading to the Diagnosis of McArdle Disease: Case Report. The Journal of hand surgery. 2015 Dec:40(12):2377-9. doi: 10.1016/j.jhsa.2015.09.015. Epub [PubMed PMID: 26612634]
Level 3 (low-level) evidenceBollig G. McArdle's disease (glycogen storage disease type V) and anesthesia--a case report and review of the literature. Paediatric anaesthesia. 2013 Sep:23(9):817-23. doi: 10.1111/pan.12164. Epub 2013 Apr 9 [PubMed PMID: 23565573]
Level 3 (low-level) evidence