Introduction
Pacemakers are adjustable artificial electrical pulse generators, frequently emitting a pulse with a duration between 0.5 and 25 ms with an output of 0.1 to 15 V at a frequency of up to 300/min. The cardiologist or pacemaker technologist will be able to interrogate and control the pacing rate, the pulse width, and the voltage, whether the device is temporary or permanent.[1] Pacemakers are typically categorized as temporary and permanent. Temporarily, pacemakers are almost always placed to stabilize the patient temporarily or facilitate some surgical procedure.[2] The implantable pacemakers are usually permanent and often significantly more complex than temporary pacemakers.[3]
The true beginning of the concept of a pacemaker began over 200 years ago. In the late 1700s, Luigi Galvani discovered that he could cause the contraction of a frog's heart simply by passing an electrical current through the heart. This concept was further realized nearly 100 years later with the first successful resuscitation of a child by Guilliame de Boulogne using electricity. He accomplished this by introducing an electrical current to the patient's chest with a return electrode on the leg after a drowning. After this feat, many successful resuscitations were reported, leading to Dr. Hyman's term "artificial cardiac pacemaker" in 1932.[4][5]
Pacemakers are one cardiac implantable electronic device type (CIED). This broad category also includes implantable cardioverter-defibrillators (ICDs). This group of devices was introduced in the 1950s, shortly after the advent of the transistor. As technology has improved, so has the pacemaker device. The first implantable ICD was developed in 1980. Since then, it has become more challenging to differentiate between pacemakers and ICDs because every ICD currently implanted has an antibradycardia pacing function.[6] The patient and any clinician should understand which device has been implanted to prevent unnecessary ICD therapy, which is most likely to occur with any electromagnetic interference and could lead to device activation with an ICD. Most types of CIED use several insulated lead wires with non-insulated tips that are implanted in the heart, either by percutaneous vein insertion or directly by a cardiac surgeon. Cardiac pacemakers comprise the pulse generator and the leads or electrodes.[1]
The North American Society of Pacing and Electrophysiology and the British Pacing and Electrophysiology Group jointly developed a generic pacemaker code utilized worldwide that would allow clinicians and manufacturers to describe the device's characteristics, which was last updated in 2002 (see Image. Pacemaker Table).[7] The first letter in the code indicates which chamber is paced; the second letter indicates which chamber is being sensed by the device; the third letter indicates if there is a response to sensing; the fourth position indicates whether the device will modulate or change the programmed rate independent of the patient's cardiac activity, for example, with exercise; the fifth and last letter of the code indicates additional multisite pacing. The last 2 letters of the code (in the fourth and fifth position) are rarely used in typical nomenclature.[7] The latest generation of pacemakers has many capabilities.[8] The simplest settings are AAI and VVI. The AAI mode paces and senses in the atrium, and each sensed event triggers the generator to fire within the P wave. The VVI mode paces and senses the ventricle and is suppressed by a sensed ventricular event.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomy and Physiology of Cardiac Conduction System
The cardiac conduction system is a specialized group of cardiac muscle cells responsible for generating and transmitting electrical impulses that coordinate heart muscle contraction. The following are the primary anatomic components of the cardiac conduction system:
-
Sinoatrial node: The sinoatrial (SA) node is the dominant pacemaker of the heart that generates the electrical impulse that travels through the atria and depolarizes the ventricles via the specialized Purkinje fibers. The SA node is an elongated, spindle-shaped structure composed of specialized cells packed in the fibrous tissue matrix and is located close to the epicardial surface of the right atrium, at the junction of the superior vena cava and the right atrium.[9] This is supplied by the SA nodal branches of the right coronary artery (55% to 60%) or the left circumference artery (35% to 40%). The SA node rarely gets blood supply from the right coronary and left circumference arteries.[10]
- Atrioventricular node: The atrioventricular node connects the atrial to the ventricles and transmits impulses from the atria to the ventricles. The compact atrioventricular node is a superficial structure located subendocardial, in the interatrial septum, at the apex of the triangle of Koch, a triangle formed by the tricuspid annulus anteriorly and the tendon of Todaro posteriorly. Branches of the right coronary artery supply the atrioventricular node in 80% to 90% of the patients. In comparison, in 10% to 20% of the people, it is supplied by the branches of the left circumference artery.[11]
- Bundle of His: The bundle of His is a thin structure with specialized conduction cells connecting the distal part of the compact atrioventricular node to the distal conduction system. This structure perforates the central fibrous body and continues through the annulus fibrosus into the interventricular septum, dividing into bundle branches. As the proximal part of the His bundle is a continuation of the atrioventricular node, the cells of the penetrating His bundle resemble those of the compact atrioventricular node, while the distal His bundle structures are identical to the proximal bundle branches.[12]
- Bundle branches and Purkinje fibers: The bundle branches originate at the superior margin of the muscular interventricular septum, immediately below the membranous septum. The right bundle branch continues into the interventricular septum as an extension of His bundle to the apex of the right ventricle and base of the anterior papillary muscle. The anatomy of the left bundle branch is variable; it divides into the anterior and posterior fascicles and gives a septal fascicle in some individuals.[13] The bundle branches divide into the Purkinje fibers, a network of fast-conducting fibers at the endocardial surface of the myocardium. These fibers transmit electrical impulses almost simultaneously to both ventricles, resulting in synchronized contraction.[14]
Indications
Indications of Permanent Pacemakers
Permanent pacemakers are indicated for individuals who have bradycardia due to sinus node dysfunction or atrioventricular block. Contemporary guidelines recommend pacemakers in the following conditions:
- Symptomatic sinus node dysfunction: A permanent pacemaker is indicated in patients with sinus node dysfunction (eg, symptomatic sinus bradycardia, chronotropic incompetence, symptomatic sinus pauses, or tachycardia-bradycardia syndrome).
-
Atrioventricular block: If a reversible cause of atrioventricular block is not identified in patients with Mobitz II atrioventricular block, advanced atrioventricular block, or complete atrioventricular block, a permanent pacemaker is indicated irrespective of symptoms.
- Atrioventricular conduction disease in the presence of neuromuscular disorders: A permanent pacemaker is indicated irrespective of symptoms in patients with neuromuscular disorders who have second-degree atrioventricular block, high-grade or third-degree atrioventricular block or distal conduction system disease with an HV interval of >70 ms.
- Permanent atrial fibrillation with bradycardia: A permanent pacemaker is indicated in patients with atrial fibrillation with a slow ventricular rate, irrespective of bradycardia-related symptoms.
-
Bradycardia due to guidelines-directed medical therapy: A permanent pacemaker is indicated in patients who develop guidelines-directed medical therapy-induced bradycardia, and no alternative medical treatment is available.
- Symptomatic first-degree or atrioventricular Wenckebach: A permanent pacemaker can be considered in symptomatic patients with gross first-degree atrioventricular block (PR >300 ms) or atrioventricular Wenckebach.
Contraindications
Though no absolute contraindications to the pacemaker implantation have been established, a transvenous permanent pacemaker is not recommended in the presence of an active infection, especially bacteremia. The other contraindications may include patient refusal and terminal illness where a pacemaker is not expected to improve quality of life. In patients whose vascular and cardiac anatomy is not favorable for a conventional transvenous pacemaker, an epicardial lead placement with thoracoscopy/thoracotomy should be considered an alternative option.[17]
Equipment
Implanting a pacemaker is a specialized procedure that requires specific equipment to ensure accuracy, safety, and efficacy. The following equipment and tools are the primary implements necessary for a pacemaker implantation procedure:
-
Pacemaker pulse generator: This device contains the pacemaker's battery and electronic circuitry; it generates electrical impulses that are delivered to the heart via the leads.
-
Pacemaker leads: These are insulated wires that carry electrical impulses from the pacemaker generator to the heart muscle. Depending on the type of pacing needed, different types of leads are available, including atrial and ventricular leads.
-
Implantation tools
- Scalpel and dissection instruments: These are used to create the incision, dissect tissues to access the implantation site, and create a pocket.
- Forceps and scissors: These instruments are used for handling tissues and cutting sutures.
- Needles and sutures: These are used to suture the leads and incision site after implantation.
-
Fluoroscopy equipment: This equipment provides real-time x-ray images of the heart and the positioning of leads during the procedure, ensuring accurate placement.
-
Electrocautery: This is used to control bleeding during the surgery by coagulating tissue and blood vessels.
-
Sterile drapes and surgical gowns and gloves: Maintain a sterile field to reduce the risk of infection during the procedure.
-
Cardiac monitoring equipment: Provides continuous monitoring of the patient's heart rhythm and vital signs throughout the procedure.
-
Anesthesia equipment: Includes medications and equipment for administering anesthesia to the patient during the implantation.
-
X-ray machine: Used in combination with fluoroscopy to visualize the heart and guide the placement of the leads.
-
Temporary pacemaker: May be considered in case of complications or if temporary pacing is needed during or after the procedure.
-
Electrocardiogram machine: Used for monitoring the patient's heart rhythm and ensuring proper function of the pacemaker postimplantation.
-
Surgical lights: Provide adequate illumination of the surgical field during the procedure.
-
Postoperative monitoring equipment: Includes equipment for monitoring the patient's recovery in the immediate postoperative period.
The operating room should also be equipped with standard surgical instruments and supplies, including sterile gauze, sponges, and irrigation solutions. Pacemaker implantation is typically performed in a specialized cardiac catheterization laboratory or an operating room equipped with all necessary monitoring and imaging capabilities to ensure the procedure's success and the patient's safety.
Personnel
Pacemaker implantation is performed by a specialized cardiologist (ie, cardiac electrophysiologist) or a cardiac surgeon. The procedure requires a team with extensive training and experience in caring for these complex patients. Other team members may include an electrophysiology fellow, an electrophysiology nurse, a technician, an anesthesiologist or anesthesia assistant, and a radiographer.
Preparation
The first step of preparation is to evaluate the indication of pacing and perform a risk-benefit analysis by taking a detailed history and doing a clinical examination of the patient. The patient should be free of infection for at least 24 hours before implant, and prophylactic antibiotics should be administered in all cases (eg, cephazolin 1 to 2 g or flucloxacillin 1 to 2 g within 1 hour of incision, or, in case of allergy, vancomycin 15 mg/kg within 90 to 120 min).[18] Patients on anticoagulation require special consideration as they are at higher risk of pocket hematoma, which increases the risk of infection. Interruption of anticoagulation can be considered in patients with non-valvular atrial fibrillation with relatively low stroke risk, while those with mechanical valves and high stroke risk can have device implants without interruption of anticoagulation, provided the International Normalized Ratio is less than 3.5.
The BRUISE-CONTROL 2 study results show no difference in hematoma in patients undergoing pacemaker implants with or without interruption of direct oral anticoagulants.[19] However, interruption of anticoagulation should be individualized based on patient characteristics and bleeding and ischemic risk. Before starting the procedure, operators should ensure all required equipment is available. Preoperative safety checks and surgical time-outs are encouraged to avoid errors. Anesthesia support should be available for potentially life-threatening complications, as well as to assist with sedation and hemodynamic support if required.
Technique or Treatment
Pocket Creation
Left-sided implants are preferred, as they are the nondominant side for most patients, and lead placement is relatively more straightforward. However, the decision should be individualized according to the specific requirements. After infiltration of local anesthetic (1% lidocaine or lidocaine mixed with bupivacaine), a horizontal (below the clavicle) or an oblique incision (parallel to the deltopectoral groove) is made.[20] The oblique incision provides better access for cephalic cutdown; however, the pocket should be created medially to minimize the migration of the device into the axilla. Dissection is carried down to the pre-pectoral fascia, creating a subcutaneous pocket. A subpectoral pocket is considered in lean individuals who do not have much subcutaneous fat to minimize pocket erosion.[21] Submuscular pockets can also be considered for cosmetic purposes and, in rare cases, to minimize the risk of Toddler syndrome in special populations.
Vascular Access
Vascular access is performed by axillary or subclavian puncture under fluoroscopy or by cephalic cutdown under direct vision. The intrathoracic subclavian vein has a higher risk of pneumothorax, so the extrathoracic subclavian or axillary vein is the preferred puncture site in the contemporary era.[22] Axillary vein puncture can be easily performed using fluoroscopic landmarks. The caudal tilt of 35 degrees helps expose the outer margin of the lung, allowing safe puncture and minimizing the risk of pneumothorax by targeting the outer margin of the first rib.[23] A venogram can be used to guide the puncture when the vein is not accessible under fluoroscopy. Cephalic cutdown avoids the risk of pneumothorax and has lower chances of lead dysfunction than subclavian access.[24] Though cephalic cutdown has a relatively higher risk of bleeding, it is not significantly different from the conventional subclavian access.[24]
Implantation of Pacing Leads
The active or passive fixation leads are implanted according to the operator's preferences; however, the active fixation leads have a lower risk of lead dislodgements than passive fixation leads. Leads are stylet-driven, and atrial leads usually come with preformed, U-shaped stylet. The right ventricular lead is usually implanted first to provide backup pacing if required and to avoid atrial lead dislodgement during ventricular lead placement. Common sites for ventricular lead implantation include the right ventricular apex and interventricular septum, while the septal right ventricular outflow tract is rarely used.[25]
Traditionally, the right ventricular apex had been the common site for right ventricular lead placement due to technical feasibility and the stable position of passive leads due to trabeculae. However, a higher risk of perforation associated with the apical position has made the interventricular septum the preferred implant site for active fixation of the right ventricular lead.[26] The tricuspid valve is crossed by modifying the straight stylet and making a curve at its distal end. A clockwise torque is used to avoid inadvertent cannulation of the coronary sinus. Ventricular ectopy and the left anterior oblique (LAO) projection can confirm the lead position in the right ventricular lead.
The same manual stylet or a different stylet curve is used to place the lead at the desired site in the right ventricle. Two orthogonal fluoroscopic projections are recommended to confirm the right ventricular lead and avoid the lead placement into the free wall of the right ventricle. Once the lead is at a desired position, the screw of the active fixation lead is deployed, and fluoroscopic markers are used to confirm the deployment. Over-rotation of the helix should be avoided as it may lead to lead dislodgement.[3]
After deployment, checking for the current of injury and testing the lead for sensed R wave amplitude and pacing threshold is recommended. The atrial lead is usually placed with a preformed U-shaped stylet, facilitating lead position into the right atrial appendage. However, a slight modification of the stylet or even lead placement at the alternate sites is required in select groups of patients when satisfactory pacing and sensing parameters or the desired position is not achieved with the conventional U-shaped stylet. After atrial lead deployment, stability should be tested by pulling the stylet back into the superior vena cava and pushing the lead toward the tricuspid valve. Both the leads should be tested for current of injury, sensed amplitude, and pacing threshold after deployment.
After placement and achieving the satisfactory parameters, leads are secured by suturing with the pectoralis muscle. Usually, the non-absorbable sutures are tied over the muscle and then over the suturing sleeves.[27] The leads are connected to the atrial and ventricular ports of the pulse generator and placed in the preformed pocket. The lead switch in the pulse generator header is an infrequent complication when atrial and ventricular leads are switched in the pulse generator and connected to the wrong port. Ideally, the serial numbers of the leads should be checked before being connected to the pulse generator to avoid the lead switch in the header.[28]
Pocket Closure
The pocket should be examined for bleeding before closure. Saline wash can be considered to clean the pocket before placing the pacemaker and leads. The pacemaker should be placed in the pocket in a way that the header is placed toward the incision to make device removal easier during pulse generator replacement. The leads should be placed under the device to minimize the chances of Toddler syndrome and minimize the damage to the leads during re-exploration and pulse generator replacement. Although pocket closure techniques vary, the closure is usually done in 2 to 3 layers. The subcutaneous tissue is commonly closed in 2 layers of 2-0 or 3-0 resorbable suture, and the subcuticular tissue and skin are closed with a braided resorbable, 4-0 suture.
Postoperative Care
Postoperative care after pacemaker implantation is crucial to ensure proper healing, prevent complications, and optimize the function of the pacemaker system.
Immediate postoperative period
In the immediate postoperative period following pacemaker implantation, careful monitoring is essential, including regular checks of vital signs such as heart rate, blood pressure, and oxygen saturation, along with continuous monitoring of the pacemaker function and heart rhythm to ensure proper pacing and sensing. Wound care is crucial, with the surgical incision site needing to be kept clean and dry and closely observed for signs of infection like redness, swelling, warmth, or drainage. While there are no specific limitations on general activity, patients should avoid strenuous activity or heavy lifting with the arm on the side of the pacemaker to prevent dislodging the leads, though the chance of this happening is minimal. Pain management instructions provided by clinicians should be tailored to the patient's comfort.
Discharge and long-term care
Education becomes a key component as patients transition to discharge and long-term care. Patients and their caregivers should be informed about the pacemaker's function, including recognizing normal versus abnormal symptoms, and advised on activity restrictions (eg, avoiding strong electromagnetic fields or engaging in vigorous contact sports). Clear instructions should be provided regarding follow-up care, including scheduled visits with a cardiologist or electrophysiologist. Patients must also understand any prescribed medications, such as antibiotics or pain management drugs, and be aware of any driving restrictions based on local regulations and their medical condition. For some, remote monitoring of the pacemaker may be available, allowing device function to be checked and issues detected early without frequent clinic visits. Encouraging a healthy lifestyle, including regular exercise as their clinician advises, a balanced diet, and smoking cessation, is also vital. Patients should be informed about when to seek emergency medical attention, such as in cases of chest pain, palpitations, dizziness, or fainting.
Follow-up visits
Follow-up visits are critical for ensuring ongoing pacemaker function. During these visits, the device's performance will be evaluated, and adjustments may be made to optimize settings. The pacemaker's battery life will also be monitored to plan for future generator replacements. Continuous education and support for the patient and caregivers about ongoing care, lifestyle modifications, and any changes in pacemaker management are essential for long-term success. The interprofessional healthcare team can help patients recover smoothly from pacemaker implantation through comprehensive postoperative care and achieve optimal long-term outcomes in managing their cardiac health.
Complications
Pacemaker implantation is generally a safe procedure with a high success rate, but like any surgical intervention, it carries some potential risks and complications. These complications can range from minor to more severe issues. Common complications associated with pacemaker implantation include:
- Arrhythmia: Nonsustained ventricular arrhythmia is commonly observed during ventricular lead placement, especially the manipulation of lead through the tricuspid valve into the right ventricular outflow tract. Sustained ventricular arrhythmia and atrial tachyarrhythmia are rarely noted during pacemaker implantation.
- Infection: Infection can occur at the surgical site or along the pathway of the leads into the heart. This can lead to localized swelling, redness, pain, and fever. The pacemaker system may be removed in severe cases, and antibiotic treatment may be required. The overall incidence of pacemakers and cardiac implantable electronic devices ranges from 0.6% to 3.4%.[18]
- Bleeding and pocket hematoma: Bleeding can occur during or after the procedure, either at the incision site or internally. Most cases are minor, but significant bleeding leading to pocket hematoma may require re-exploration of the pocket. The incidence of pocket hematoma varies widely, from <0.5% to as high as 16%.[3] Pocket hematoma increases the risk of pacemaker infection.
- Lead-related complications:
- Lead dislodgement: Leads can move from their intended position, causing improper pacing or failure to sense the heart's electrical activity correctly.
- Lead fracture: Leads can break or fracture, which may lead to malfunction of the pacemaker system.
- Venous thrombosis: Blood clots forming in the vein where the leads are placed can impede blood flow.
- Pneumothorax: A puncture of the lung tissue during the insertion of leads, leading to the accumulation of air in the chest cavity. This may require drainage.
- Cardiac perforation: Rarely, the leads can puncture the heart chambers or other structures within the chest cavity. The true incidence of lead perforation can not be estimated due to the variable definitions; the reported range of perforation varies from <0.1% to as high as 1.5%. Lead perforation is usually reported in the first 4 weeks of implant, rarely occurs in the later period, and is even reported years after the implant.[3]
- Allergic reaction: Rarely, patients may be allergic to materials used in the pacemaker system, such as metal alloys or medications.
- Device-related complications
- Battery depletion: The pacemaker battery has a limited lifespan (usually up to 10 years), after which it needs to be replaced.
- Device malfunction: Rarely, the pacemaker may malfunction, requiring replacement or reprogramming.
- Psychological impact: Some patients may experience anxiety, depression, or adjustment issues related to having a pacemaker implanted.
- Long-term complications: Over time, there is a small risk of complications such as lead insulation breakage, lead calcification, or infection of the device pocket.
The overall risk of complications is relatively low, and many patients experience significant improvement in their quality of life with a properly functioning pacemaker. Clinicians carefully assess each patient's risk factors and monitor them closely before, during, and after the procedure to minimize the likelihood of complications.
Clinical Significance
Pacemakers are of significant clinical importance in cardiology due to their ability to treat and manage various cardiac rhythm disorders. The clinical significance of pacemakers includes:
- Bradycardia treatment
- Pacemakers are primarily used to treat bradycardia, which can lead to symptoms such as dizziness, fainting, fatigue, and shortness of breath. Pacemakers help maintain a normal heart rate and improve bradycardia-related symptoms.
- Heart block management
- Heart block is a condition in which the electrical signals from the atria to the ventricles are delayed or blocked.
- Pacemakers can effectively bypass these blockages by delivering electrical impulses directly to the ventricles or maintaining appropriate timing between atrial and ventricular contractions.
- Improvement in quality of life
- Pacemakers can significantly improve the quality of life for patients with symptomatic bradycardia or heart block by reducing symptoms such as fatigue, fainting episodes, and shortness of breath.
- They enable patients to engage in normal daily activities and exercise without limitations imposed by their heart rhythm disorder.
- Syncope and sudden cardiac arrest prevention
- Pacemakers help prevent dangerous complications associated with severe bradycardia, such as syncope (fainting) or even sudden cardiac arrest in some cases.
- By maintaining a stable heart rate, pacemakers reduce the risk of life-threatening arrhythmias.
- Versatility in management
- Pacemakers can be programmed and adjusted to meet individual patient needs, including variations in heart rate requirements during rest and physical activity.
- Advanced pacemaker models may include additional features such as rate response algorithms to increase heart rate during exercise.
- Technological advancements
- Continuous advancements in pacemaker technology have improved device longevity, reduced complications, and enhanced monitoring capabilities through remote monitoring systems.
- These advancements contribute to better management and outcomes for patients requiring pacemakers.
- Indications beyond bradycardia
- Pacemakers may also be used in certain cases of heart failure (eg, cardiac resynchronization therapy) or to manage specific arrhythmias refractory to other treatments.
- They play a role in optimizing cardiac function and improving overall heart health in selected patient populations.
Overall, pacemakers represent a critical therapeutic intervention for patients with various cardiac rhythm disorders. They offer significant clinical benefits by maintaining appropriate heart rate and rhythm, improving symptoms, and reducing the risk of serious complications associated with bradycardia and heart block.
Enhancing Healthcare Team Outcomes
Effective postoperative care following pacemaker implantation requires a coordinated, interprofessional approach to enhance patient-centered care, outcomes, safety, and team performance. Advanced clinicians, nurses, pharmacists, and other health professionals must collaborate seamlessly, focusing on vital signs and cardiac rhythm monitoring to ensure proper pacemaker function. Physicians lead in strategizing follow-up care, while nurses handle wound care, patient education, and early detection of complications. Pharmacists contribute to pain management, medication adherence, and educating patients on activity restrictions. Communication among all team members ensures cohesive care, remote monitoring integration, and prompt interventions, fostering patient safety and optimal recovery.
Media
(Click Image to Enlarge)
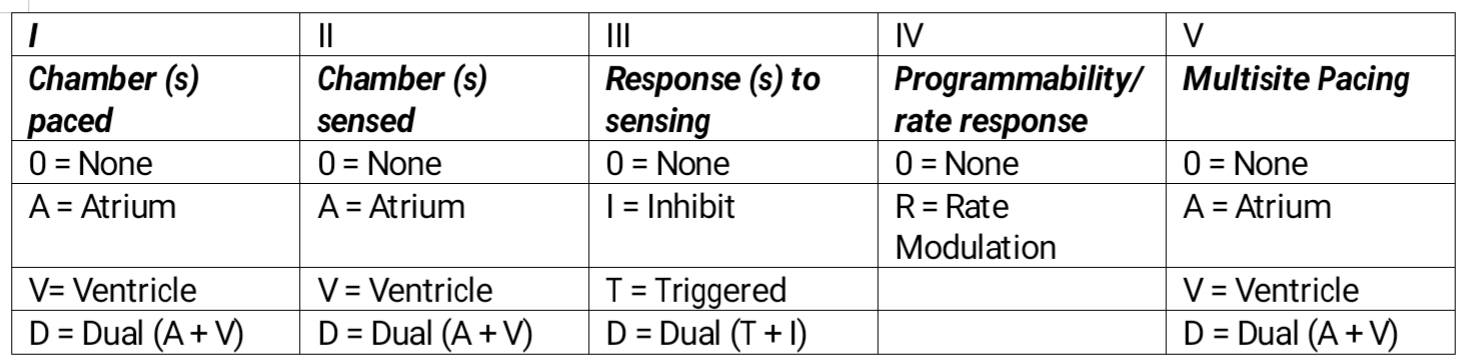
Pacemaker Table. External pacing is the fastest available method to synchronize cardiac rhythm in all the bradyarrhythmias indicated by the American Heart Association. This temporary method is used to maintain cardiac output in irreversible conditions where a permanent pacemaker is needed or in reversible situations where permanent pacing is contraindicated.
Contributed by M Ellison, MD, FASA
References
Mulpuru SK, Madhavan M, McLeod CJ, Cha YM, Friedman PA. Cardiac Pacemakers: Function, Troubleshooting, and Management: Part 1 of a 2-Part Series. Journal of the American College of Cardiology. 2017 Jan 17:69(2):189-210. doi: 10.1016/j.jacc.2016.10.061. Epub [PubMed PMID: 28081829]
Loehry JK. Temporary cardiac pacing. Postgraduate medical journal. 2000 Mar:76(893):189 [PubMed PMID: 10928911]
Burri H, Starck C, Auricchio A, Biffi M, Burri M, D'Avila A, Deharo JC, Glikson M, Israel C, Lau CP, Leclercq C, Love CJ, Nielsen JC, Vernooy K, Reviewers:, Dagres N, Boveda S, Butter C, Marijon E, Braunschweig F, Mairesse GH, Gleva M, Defaye P, Zanon F, Lopez-Cabanillas N, Guerra JM, Vassilikos VP, Martins Oliveira M. EHRA expert consensus statement and practical guide on optimal implantation technique for conventional pacemakers and implantable cardioverter-defibrillators: endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), and the Latin-American Heart Rhythm Society (LAHRS). Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2021 Jul 18:23(7):983-1008. doi: 10.1093/europace/euaa367. Epub [PubMed PMID: 33878762]
Level 3 (low-level) evidenceCrofoot M, Sarwar A, Weir AJ. External Pacemaker. StatPearls. 2024 Jan:(): [PubMed PMID: 30137851]
Ivanchina AE, Kopylov FY, Volkova AL, Samojlenko IV, Syrkin AL. [Clinical Value of Algorithms of Minimization of Right Ventricular Pacing in Patients With Sick Sinus Syndrome and History of Atrial Fibrillation]. Kardiologiia. 2018 Aug:(8):58-63 [PubMed PMID: 30131043]
Matchett M, Sears SF, Hazelton G, Kirian K, Wilson E, Nekkanti R. The implantable cardioverter defibrillator: its history, current psychological impact and future. Expert review of medical devices. 2009 Jan:6(1):43-50. doi: 10.1586/17434440.6.1.43. Epub [PubMed PMID: 19105779]
Bernstein AD, Daubert JC, Fletcher RD, Hayes DL, Lüderitz B, Reynolds DW, Schoenfeld MH, Sutton R. The revised NASPE/BPEG generic code for antibradycardia, adaptive-rate, and multisite pacing. North American Society of Pacing and Electrophysiology/British Pacing and Electrophysiology Group. Pacing and clinical electrophysiology : PACE. 2002 Feb:25(2):260-4 [PubMed PMID: 11916002]
Świerżyńska E, Oręziak A, Główczyńska R, Rossillo A, Grabowski M, Szumowski Ł, Caprioglio F, Sterliński M. Rate-Responsive Cardiac Pacing: Technological Solutions and Their Applications. Sensors (Basel, Switzerland). 2023 Jan 27:23(3):. doi: 10.3390/s23031427. Epub 2023 Jan 27 [PubMed PMID: 36772467]
Ho SY, Sánchez-Quintana D. Anatomy and pathology of the sinus node. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2016 Jun:46(1):3-8. doi: 10.1007/s10840-015-0049-6. Epub 2015 Aug 30 [PubMed PMID: 26319648]
Nerantzis CE, Anninos H, Koutsaftis PN. Variation in the blood supply of the sinus node. Surgical and radiologic anatomy : SRA. 2010 Dec:32(10):983-4. doi: 10.1007/s00276-010-0635-3. Epub 2010 Feb 16 [PubMed PMID: 20157710]
Anderson RH, Ho SY. The architecture of the sinus node, the atrioventricular conduction axis, and the internodal atrial myocardium. Journal of cardiovascular electrophysiology. 1998 Nov:9(11):1233-48 [PubMed PMID: 9835269]
von Knorre GH. The 125th anniversary of the His bundle discovery. Herzschrittmachertherapie & Elektrophysiologie. 2018 Mar:29(1):116-121. doi: 10.1007/s00399-018-0554-2. Epub 2018 Jan 17 [PubMed PMID: 29344737]
Massing GK, James TN. Anatomical configuration of the His bundle and bundle branches in the human heart. Circulation. 1976 Apr:53(4):609-21 [PubMed PMID: 1253382]
Sedmera D, Gourdie RG. Why do we have Purkinje fibers deep in our heart? Physiological research. 2014:63(Suppl 1):S9-18 [PubMed PMID: 24564668]
Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, Barrabés JA, Boriani G, Braunschweig F, Brignole M, Burri H, Coats AJS, Deharo JC, Delgado V, Diller GP, Israel CW, Keren A, Knops RE, Kotecha D, Leclercq C, Merkely B, Starck C, Thylén I, Tolosana JM, Leyva F, Linde C, Abdelhamid M, Aboyans V, Arbelo E, Asteggiano R, Barón-Esquivias G, Bauersachs J, Biffi M, Birgersdotter-Green U, Bongiorni MG, Borger MA, Čelutkienė J, Cikes M, Daubert JC, Drossart I, Ellenbogen K, Elliott PM, Fabritz L, Falk V, Fauchier L, Fernández-Avilés F, Foldager D, Gadler F, De Vinuesa PGG, Gorenek B, Guerra JM, Hermann Haugaa K, Hendriks J, Kahan T, Katus HA, Konradi A, Koskinas KC, Law H, Lewis BS, Linker NJ, Løchen ML, Lumens J, Mascherbauer J, Mullens W, Nagy KV, Prescott E, Raatikainen P, Rakisheva A, Reichlin T, Ricci RP, Shlyakhto E, Sitges M, Sousa-Uva M, Sutton R, Suwalski P, Svendsen JH, Touyz RM, Van Gelder IC, Vernooy K, Waltenberger J, Whinnett Z, Witte KK. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2022 Jan 4:24(1):71-164. doi: 10.1093/europace/euab232. Epub [PubMed PMID: 34455427]
Kusumoto FM, Schoenfeld MH, Barrett C, Edgerton JR, Ellenbogen KA, Gold MR, Goldschlager NF, Hamilton RM, Joglar JA, Kim RJ, Lee R, Marine JE, McLeod CJ, Oken KR, Patton KK, Pellegrini CN, Selzman KA, Thompson A, Varosy PD. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. Journal of the American College of Cardiology. 2019 Aug 20:74(7):932-987. doi: 10.1016/j.jacc.2018.10.043. Epub 2018 Nov 6 [PubMed PMID: 30412710]
Level 1 (high-level) evidenceLichtenstein BJ, Bichell DP, Connolly DM, Lamberti JJ, Shepard SM, Seslar SP. Surgical approaches to epicardial pacemaker placement: does pocket location affect lead survival? Pediatric cardiology. 2010 Oct:31(7):1016-24. doi: 10.1007/s00246-010-9754-1. Epub 2010 Aug 6 [PubMed PMID: 20690018]
Blomström-Lundqvist C, Traykov V, Erba PA, Burri H, Nielsen JC, Bongiorni MG, Poole J, Boriani G, Costa R, Deharo JC, Epstein LM, Saghy L, Snygg-Martin U, Starck C, Tascini C, Strathmore N, ESC Scientific Document Group. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2020 Apr 1:22(4):515-549. doi: 10.1093/europace/euz246. Epub [PubMed PMID: 31702000]
Level 3 (low-level) evidenceBirnie DH, Healey JS, Wells GA, Ayala-Paredes F, Coutu B, Sumner GL, Becker G, Verma A, Philippon F, Kalfon E, Eikelboom J, Sandhu RK, Nery PB, Lellouche N, Connolly SJ, Sapp J, Essebag V. Continued vs. interrupted direct oral anticoagulants at the time of device surgery, in patients with moderate to high risk of arterial thrombo-embolic events (BRUISE CONTROL-2). European heart journal. 2018 Nov 21:39(44):3973-3979. doi: 10.1093/eurheartj/ehy413. Epub [PubMed PMID: 30462279]
Lokhandwala D, Gupta A, Desai V, Panicker GK, Vora A. A pilot study comparing two sites for incision during pacemaker implantation and their influence on the scar. Indian heart journal. 2018 Sep-Oct:70(5):704-708. doi: 10.1016/j.ihj.2018.05.008. Epub 2018 May 9 [PubMed PMID: 30392510]
Level 3 (low-level) evidenceVandenberk B, Murray K, Rizkallah J. Risk Mitigation of Pacemaker Pocket Erosion in Thin Patients. CJC open. 2022 Jun:4(6):585-587. doi: 10.1016/j.cjco.2022.03.002. Epub 2022 Mar 9 [PubMed PMID: 35734518]
Liu P, Zhou YF, Yang P, Gao YS, Zhao GR, Ren SY, Li XL. Optimized Axillary Vein Technique versus Subclavian Vein Technique in Cardiovascular Implantable Electronic Device Implantation: A Randomized Controlled Study. Chinese medical journal. 2016 Nov 20:129(22):2647-2651. doi: 10.4103/0366-6999.193462. Epub [PubMed PMID: 27823994]
Level 1 (high-level) evidenceYang F, Kulbak G. A new trick to a routine procedure: taking the fear out of the axillary vein stick using the 35° caudal view. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2015 Jul:17(7):1157-60. doi: 10.1093/europace/euv066. Epub 2015 May 11 [PubMed PMID: 25969438]
Benz AP, Vamos M, Erath JW, Hohnloser SH. Cephalic vs. subclavian lead implantation in cardiac implantable electronic devices: a systematic review and meta-analysis. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2019 Jan 1:21(1):121-129. doi: 10.1093/europace/euy165. Epub [PubMed PMID: 30020452]
Level 1 (high-level) evidenceBongiorni MG, Proclemer A, Dobreanu D, Marinskis G, Pison L, Blomstrom-Lundqvist C, Scientific Initiative Committee, European Heart Rhythm Association. Preferred tools and techniques for implantation of cardiac electronic devices in Europe: results of the European Heart Rhythm Association survey. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2013 Nov:15(11):1664-8. doi: 10.1093/europace/eut345. Epub [PubMed PMID: 24170423]
Level 3 (low-level) evidenceCano Ó, Andrés A, Alonso P, Osca J, Sancho-Tello MJ, Olagüe J, Martínez-Dolz L. Incidence and predictors of clinically relevant cardiac perforation associated with systematic implantation of active-fixation pacing and defibrillation leads: a single-centre experience with over 3800 implanted leads. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2017 Jan:19(1):96-102. doi: 10.1093/europace/euv410. Epub 2016 Feb 3 [PubMed PMID: 26847075]
Level 1 (high-level) evidenceRezazadeh S, Wang S, Rizkallah J. Evaluation of common suturing techniques to secure implantable cardiac electronic device leads: Which strategy best reduces the lead dislodgement risk? Canadian journal of surgery. Journal canadien de chirurgie. 2019 Feb 1:62(1):E7- [PubMed PMID: 30694034]
Jastrzebski M. Pacemaker malfunction due to atrial and ventricular leads switched in the header: two faces of the same mistake? Pacing and clinical electrophysiology : PACE. 2008 Jun:31(6):733-5. doi: 10.1111/j.1540-8159.2008.01078.x. Epub [PubMed PMID: 18507547]