Indications
The discovery of phosphodiesterase 5 inhibitors (PDE5 inhibitors) for causing the erection of the penis was accidental, noticed as a side effect while being administered to investigate their ability to treat hypertension and angina. Erectile dysfunction has become an extremely prevalent concern, with recent figures estimating that about 320 million will encounter the disorder by 2025.[1] There are several available PDE5 inhibitors: sildenafil, vardenafil, tadalafil, and avanafil, which are FDA approved; lodenafil, udenafil, and mirodenafil are the other non-FDA commercially available drugs.
- Erectile Dysfunction: They are recommended as the first-line treatment for ED due to psychogenic, vascular, and neuropathic causes when combined with etiology-specific therapy.
- Idiopathic Pulmonary Hypertension: Abundant PDE-5 receptors in the pulmonary vasculature make PDE5 inhibitors important for managing pulmonary hypertension. These drugs are preferred in patients with NYHA class 2 or 3 with negative acute vasodilator response. They are not indicated in patients with NYHA class 4, where prostacyclin agonists like epoprostenol and iloprost are more appropriate.
- Premature Ejaculation (PE) associated with erectile dysfunction: PDE5 inhibitors effectively manage premature ejaculation associated with erectile dysfunction but not in patients with PE alone. PDE5 receptors get expressed throughout the contractile tissue of the male reproductive tract and the accessory glands, and their inhibition increases the ejaculatory latency.
- High Altitude Illness: Treatment with sildenafil has been shown to reduce the incidence of pulmonary hypertension in people with altitude-induced high pulmonary systolic arterial pressure, but no improvement in arterial oxygen saturation, heart rate, and acute mountain sickness.[2]
- Penile Rehabilitation after Radical Prostatectomy: Early use of sildenafil after radical prostatectomy has been found beneficial in treating ED post RP due to neuro-regenerative effects on the cavernous nerve, which usually gets damaged in the procedure.
- Antianginal: Brought into the market as an antianginal initially, these drugs, through strong evidence obtained from certain studies, have been shown to reduce mortality due to major cardiovascular events in people with diabetes through their effects on endothelial function.[3] Although they play a role in preventing coronary events, they are currently not used for this purpose.
- Lower Urinary Tract Symptoms (LUTS): LUTS precipitates due to benign prostatic hyperplasia (BPH) with simultaneous erectile dysfunction. These drugs reduce the symptoms of hesitancy, urgency, and frequency due to an obstructive cause in patients with the simultaneous presence of ED. These drugs have not shown any advantage in combating LUTS symptoms alone. When used in combination with alpha-blockers, they had similar or inferior outcomes compared to alpha-blockers alone.[4]
Following are the indications where emerging evidence has revealed the advantages of using PDE5 inhibitors, but more research, particularly on human subjects, is necessary to understand their efficacy:
- Heart Failure: PDE5 inhibitors have reduced cardiac hypertrophy in mouse and canine models. Due to the presence of PDE5 receptors in myocardial tissue, their manipulation can subsequently be beneficial for modifying the progression of numerous heart diseases.[5] PDE5 receptors are also expressed in normal myocardium, and their expression increases significantly in dilated cardiomyopathy, right ventricular hypertrophy, and pulmonary hypertension. Taking a setback in the management of heart failure, the largest trial (RELAX), conducted to study the benefits of PDE5 inhibitors in patients with heart failure with preserved ejection fraction, found no improvement in functional outcome and clinical status the patients.[6]
- Stroke: Recent animal studies have observed decreased infarct size and increased protection against ischemic reperfusion injury by markedly increasing cGMP levels and angiogenesis if PDE5 inhibitors are administered 24 hours after stroke.[7] Administration of PDE5 inhibitors has been shown to improve neural growth and short-term memory, therefore potentially reversing the effects of decreased cGMP levels observed in aging. A study aimed at measuring cerebral blood flow found no change in the blood velocity using PDE5 inhibitors. Still, it increased blood velocity in patients with erectile dysfunction, pulmonary hypertension, and other diseases with an impaired endothelial dilatory response.[8]
- Peripheral neuropathy: A report was published suggesting that daily use of PDE5 inhibitors, through improved blood flow through vasa vasorum, helped alleviate peripheral neuropathy symptoms.
- Improving fertility- Oral administration of PDE5Is has been shown to increase the motility of sperms in infertile men with oligospermia but, surprisingly, did not affect normal patients.[9]
- Peripheral Arterial Disease (PAD): Chronic administration of PDE5 inhibitors has shown to improve walking distance in patients with the peripheral arterial disease (PAD), likely through manipulating the NO pathway. It has also demonstrated a reduction in the incidence of digital ulcers in patients with systemic sclerosis.
- Diabetic Nephropathy: PDE5 inhibitor's role in diabetic nephropathy has been the target of a few studies through improving insulin sensitivity and reducing the severity of albuminuria observed in nephropathy.[3]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
To understand the mechanism of action of PDE5 inhibitors, one must first understand the normal physiology of penile erection, an area of medicine where most PDE5 inhibitors are currently in use. After sexual stimulation, nerve impulses release neurotransmitters in the corpora cavernosa, causing the production of nitric oxide by endothelial cells, which diffuses into the adjacent smooth muscle cells and stimulates the formation of cGMP, leading to vasodilation and increased penile blood flow.
Mechanism of PDE-5 Inhibitors on cGMP
These drugs inhibit the enzyme phosphodiesterase-5 (PDE-5) present in the smooth muscle cells of the vessels. By inhibiting this enzyme, these drugs prevent the degradation of cGMP by PDE-5. GMP can cause activation of protein kinase G, leading to relaxation of the vascular smooth muscle. Prevention of degradation of cGMP by PDE-5 leads to the accumulation of cGMP in the vascular smooth muscle, thereby leading to dilatation of the blood vessels through phosphorylation of different downstream effector molecules. Dilatation of the penile arteries leads to a more prolonged erection. In addition, PDE5Is improve endothelial function and reduce apoptosis of vascular smooth muscle cells in the corpus cavernosum.[10]
A similar mechanism of action has also been shown to result in vasodilation of the pulmonary arteries, relieving pulmonary hypertension symptoms. They also inhibit the remodeling of the pulmonary vasculature. When given to subjects suffering from heart failure, they have been known to inhibit the remodeling of the myocardium. All the PDE5 inhibitors mentioned above have the same mechanism of action. Still, they differ in their PDE isozyme selectivity with PDE6 (sildenafil), and PDE11 (tadalafil) is also affected by the cross-reactivity, leading to the presentation of specific side effects associated with PDE5 inhibitor use.
Administration
The following dose of PDE inhibitors is usually recommended for the treatment of erectile dysfunction:[11]
- Sildenafil: 25 mg to 100 mg orally administered 1 hour before intercourse
- Tadalafil: 5 mg to 20 mg orally administered 1 hour before intercourse
- Vardenafil: 10 mg to 20 mg orally administered 1 hour before intercourse
- Some clinicians and researchers recommend chronic daily use of low-dose PDE5 inhibitors. They have increased penile blood flow and improved endothelial function, in addition to a reduction of apoptosis of vascular smooth muscle cells in the corpus cavernosum.
The oral doses of PDE5 inhibitors recommended for the treatment of pulmonary arterial hypertension (PAH):
- Sildenafil 20 mg three times daily
- Tadalafil 40 mg once daily
For patients with lower urinary tract symptoms of benign prostatic hyperplasia (BPH) with concomitant ED, tadalafil 5 mg is preferred. Characteristics of different types of PDE5Is appear in Table 1.
Adverse Effects
None of the PDE5 inhibitors are genuinely selective for the receptor PDE5, and most of the harmful effects occur due to cross-reactivity with other PDE isoenzymes. These effects are usually dose-dependent. Some of the common adverse effects encountered with the administration of PDE5Is are:[12]
- Mild headache
- Flushing - experienced more with sildenafil
- Dyspepsia
- Altered color vision presenting as a slight and transient blue tinge to the vision - the presence of a high concentration of PDE6 enzyme in rods and cones of retina makes these cells a susceptible target for PDE5 inhibitors, especially with sildenafil which has a high affinity for inhibiting PDE6 in addition to PDE5. This effect has not been shown to be accompanied by any structural and functional changes in the retina.
- Back pain and myalgias - due to a high concentration of PDE 11 enzyme in skeletal muscle, which shows significant cross-reactivity with tadalafil.
- Hypotension and dizziness
- Rhinitis
Nevertheless, the adverse outcomes encountered with PDE5 inhibitors rarely lead to their discontinuation.
PDE5Is use has also correlated with specific less known, rarely encountered side effects, and the low frequency of the occurrence of these adverse effects does not necessitate the withdrawal of the drugs from the market-
- NAION (Non-arteritic anterior ischemic optic neuropathy) and painless decrease in vision in one eye, which is usually irreversible. Its pathophysiology is unknown, but it shows an increased incidence in patients with hypertension, diabetes, hyperlipidemia, and cardiovascular disease.
- Hearing loss - Sensorineural hearing loss due to unclear pathophysiology has been observed in a few case studies, prompting the FDA to issue a warning about hearing loss from using PDE5I.
- Priapism occurs infrequently, but the risk increases if concomitantly used with other ED meds. Some recent studies have documented using PDE5 inhibitors daily to prevent the development of this rare occurrence of priapism.[13]
- Melanoma - Emerging studies have focused interest on the risk of melanoma with chronic administration of PDE5Is.[14] There is a hypothesis that low levels of PDE5I through mitogen-activated protein kinase can increase the risk, especially in patients with BRAF gene mutation.
- Prostate cancer
- In some recent studies, researchers have noted an incidence of prostate cancer recurrence after radical prostatectomy, but the data is not substantial enough to require their discontinuation in these patients.
Contraindications
Absolute Contraindications
- In patients taking nitrates or nitroglycerin, concomitant use of PDE5 inhibitors leads to excessive preload reduction. This phenomenon is common in patients using long-acting nitrates like isosorbide mononitrate, isosorbide dinitrate, and transdermal nitroglycerin patches as prophylaxis for chronic angina concomitantly initiating PDE5 inhibitors. American College of Cardiology recommends patients taking PDE5Is to wait for at least 1 to 2 days after the last PDE5I dose before administering nitrates.[1]
- Vardenafil is known to cause minor QT prolongation and is, therefore, contraindicated in patients taking type 1A, type 3 antiarrhythmics, and patients with congenital prolonged QT syndrome.[15]
Caution is Necessary for Patients with the Following Relative Contraindications
- History of MI, stroke, or life-threatening arrhythmia in the past six months
- Resting hypotension or hypertension
- History of heart failure or unstable angina
- Concomitant administration of alpha-blockers
Monitoring
Certain drugs like nitrates are absolutely contraindicated in patients taking PDE5 inhibitors, and therefore ED patients should be advised about not administering the two drugs concomitantly. Co-administration of PDE5 inhibitors and nitrates is contraindicated, but thorough hemodynamic monitoring is necessary if the need arises. Some medications like alpha-blockers are needed to relieve concomitant symptoms of BPH in patients with ED and, therefore, require caution with frequent monitoring of blood pressure levels and prompt arrangement of an appointment with a physician if hypotensive symptoms present, which may necessitate discontinuation of PDE5 inhibitor. PDE5 inhibitors should only be administered in stable patients taking alpha-blockers. Proper titration and increased dosing in a stepwise fashion if co-administered with alpha-blockers.
Patients should consult a physician if they encounter a sustained erection persisting for more than 4 hours, as prolonged blood engorgement of blood in the penis can compromise the arterial supply and lead to penile necrosis.
If patients experience an inadequate response to treatment with a PDE5 inhibitor, consider direct injections of PGE1, papaverine, phentolamine, or a combination in patients with intact vasculature. If still no response, get duplex Doppler ultrasonography, penile cavernosography, and pudendal arteriography to recognize the cause of refractory ED.
All the PDE5 inhibitors undergo extensive tubular reabsorption in the kidney and get extensively excreted as metabolites in the stool. Nonetheless, in patients with severe renal insufficiency (CrCl less than 30 ml/min), where the presence of concomitant ED is fairly common, with some studies reporting prevalence rates as high as 80% in patients undergoing dialysis,[16] it is advisable to initiate PDE5 inhibitor therapy at the lowest dose possible with gradual up-titration.[17]
PDE5 inhibitors undergo rapid metabolism in the liver, most notably through the CYP3A pathway. Similar to the recommendations for using PDE5 inhibitors in renal dysfunction, impairment of hepatic function also warrants starting lower doses and gradual up-titration while monitoring for adverse effects. Regularly scheduled follow-ups and frequent monitoring for side effects should take place.
Toxicity
No evidence has emerged concerning developing any form of dependence or tolerance with the chronic use of PDE5 inhibitors. Some recent reports have found them misused concomitantly with alcohol and illicit drugs. A few case reports of seizures and myocardial infarction with the administration of PDE5 inhibitors have come forward, likely due to cerebral vasodilatory and cytochrome P450 inhibition of the illicit drugs that are sometimes taken concurrently with the meds.[18][19]
A case study was conducted on a middle-aged man who consumed 24 tablets of 100 mg sildenafil and presented with transient visual complications, except for a visual field defect and annular scotoma that chronically persisted.[20]
Enhancing Healthcare Team Outcomes
Managing the Underlying Cause
Erectile dysfunction can be due to multiple reasons – psychogenic, neurogenic, vascular, or hormonal. Therefore, therapy with symptomatic management with PDE5 inhibitors should be accompanied by simultaneous removal of the etiology causing ED. Hence it is crucial to obtain a relevant history and perform an appropriate physical examination.
Patients with psychogenic causes of ED usually have typical early morning and nocturnal erections but cannot achieve or maintain an erection during a sexual encounter with a specific partner. These patients will benefit from counseling and a referral to a psychiatrist if unremitting symptoms are present.
It is essential to identify atherosclerotic risk factors like smoking, hypertension, diabetes mellitus, and hyperlipidemia in patients presenting with a vascular cause of ED. In addition to the absence of nocturnal and early morning erections, these patients may present with symptoms of atherosclerosis of major blood vessels, particularly angina, claudication, or a history of a significant cardiovascular event. Therefore, it is recommended to monitor blood pressure, blood glucose, HbA1C, and lipid levels and initiate treatment for the underlying cause. In addition, patients should be counseled on the importance of smoking cessation and maintaining appropriate dietary and lifestyle habits. ED patients with concomitant history of long-standing diabetes should be monitored for their diabetic status and frequent neurological examinations to check for autonomic neuropathy. Patients with hormonal causes of ED present with reduced libido, suggesting hypogonadism as the cause of ED, which is manageable accordingly.
Treating the underlying cause of ED can have a tremendous impact on the resolution of symptoms without the need to administer PDE5 inhibitors. Concomitant administration of statins, anti-oxidants, and testosterone supplements may alleviate the condition. Careful attention should be given to ED patients with comorbidities like hypertension, diabetes, and hyperlipidemia because it has been observed that strict control of blood pressure, glucose, and lipid profile accentuates the sensitivity of ED to PDE5 inhibitors.
As the above exemplifies, covering all aspects of ED and using PDE5 inhibitors requires an interprofessional team approach. All the clinicians listed above are candidates for starting therapy for their patients, but they need to work collaboratively across disciplines to ensure safe treatment and minimal adverse effects. The pharmacist should also have significant involvement, checking for drug-drug interactions, verifying dosing based on the issue (ED vs. pulmonary HTN), and counseling the patients on proper dosing and administration. Nursing can also help assess treatment effectiveness and patient compliance. Both pharmacists and nurses need to be able to contact the prescriber with any concerns they may encounter. As clinicians, specialists, nurses, and pharmacists all take an active, collaborative role, PDE5 inhibitor therapy can be most effective for patients with minimal adverse effects. [Level 5]
Expansion of Utilities for PDE5 Inhibitors
Heart Diseases
There appear to be new emerging benefits of PDE5 inhibitors in managing heart failure and preventing myocardial remodeling post-infarction. The advantages of using PDE5 inhibitors in these diseases need to be studied extensively for inclusion in the treatment plans for these conditions.
Oncology
Due to the increased expression of PDE5 receptors on tumor cells, including colon, breast, lung, bladder, and prostate, these drugs have shown a positive response through increasing apoptosis of cancerous cells and blocking one or more Multidrug-resistant transporters such as P-glycoproteins.
Diabetes Mellitus
One study through the chronic administration of PDE5 inhibitors, particularly tadalafil, produced a promising result in reducing pro-inflammatory cytokine levels in patients with type 2 diabetes.[3]
Angina
For patients with co-existent angina, a new drug is available in the market known as ranolazine, which is indicated for prophylactic treatment in chronic angina in patients refractory to first-line antianginal drugs like nitrate and beta-blockers with an added advantage of being safely co-administered with PDE5 inhibitors.
Improving Drug Administration
The most vital modality to enhancing efficacy and compliance of PDE5 inhibitors involves providing instructions to the patients regarding appropriate administration and the possible adverse effects associated with taking PDE5 inhibitors. Since about 30 to 35% of patients do not respond to on-demand administration of PDE5 inhibitors, chronic daily administration of these medications can be considered a reasonable alternative to induce normal sexual functioning with the added advantage of not exhibiting tachyphylaxis.
A new type of oro-dispensable sildenafil formulation is on the market, which disintegrates within seconds of ingestion and is absorbed quickly in the mouth. This formulation offers an advantage in patients with dysphagia and improves adherence due to rapid effects.[21]
As an epilogue, the role of PDE5 inhibitors, especially sildenafil and tadalafil, has been well established clinically in erectile dysfunction and pulmonary hypertension. Nevertheless, these drugs offer tremendous potential in other areas of medicine like heart failure, peripheral neuropathy, and peripheral arterial disease, which requires extensive research before entering the market for the treatment of these disorders.
Media
(Click Image to Enlarge)
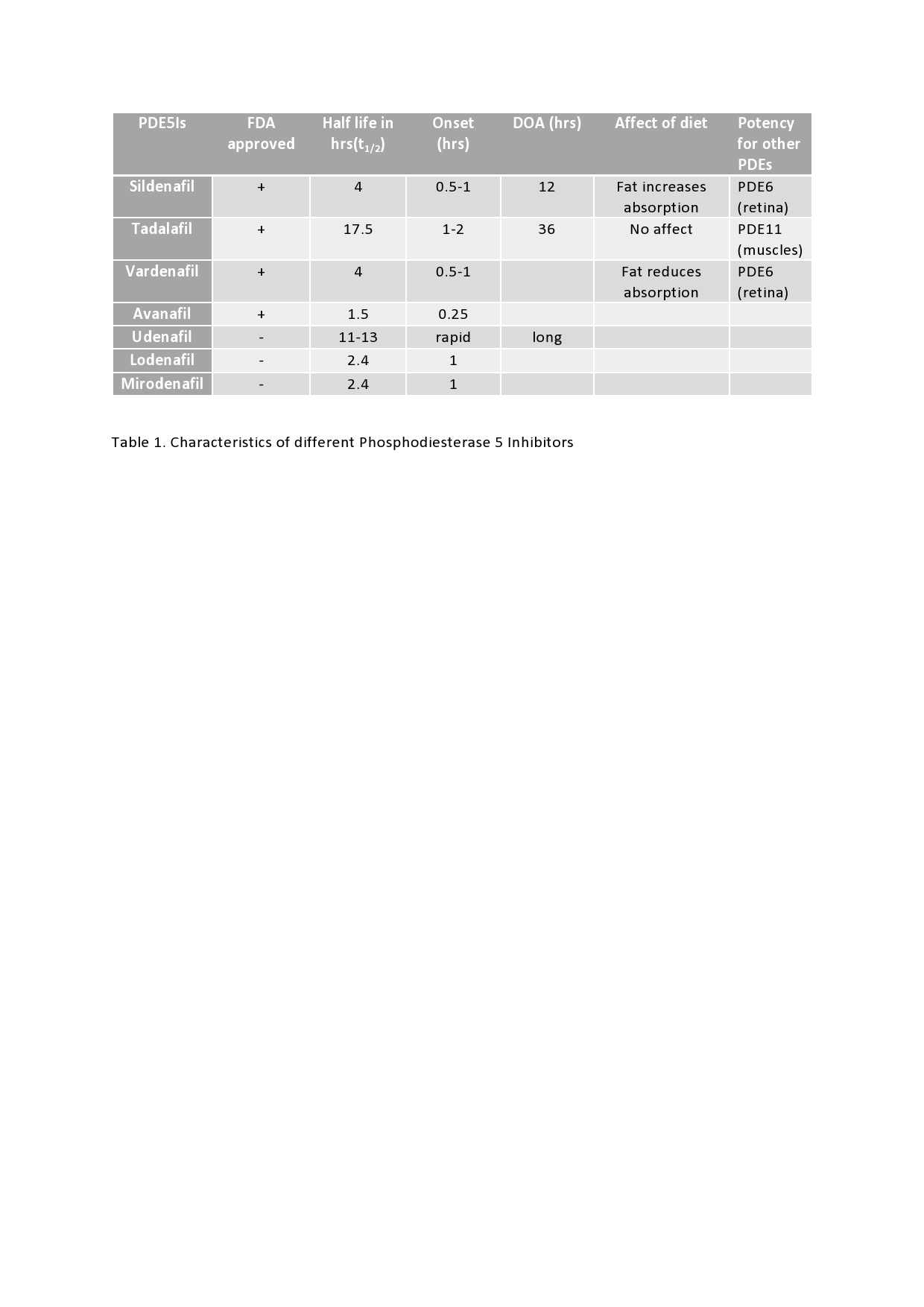
Characteristics of different Phosphodiesterase 5 Inhibitors Contributed by Armaan Dhaliwal
References
Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU international. 1999 Jul:84(1):50-6 [PubMed PMID: 10444124]
Xu Y, Liu Y, Liu J, Qian G. Meta-analysis of clinical efficacy of sildenafil, a phosphodiesterase type-5 inhibitor on high altitude hypoxia and its complications. High altitude medicine & biology. 2014 Apr:15(1):46-51. doi: 10.1089/ham.2013.1110. Epub [PubMed PMID: 24673534]
Level 1 (high-level) evidenceHong JH, Kwon YS, Kim IY. Pharmacodynamics, pharmacokinetics and clinical efficacy of phosphodiesterase-5 inhibitors. Expert opinion on drug metabolism & toxicology. 2017 Feb:13(2):183-192. doi: 10.1080/17425255.2017.1244265. Epub 2016 Oct 21 [PubMed PMID: 27690667]
Level 3 (low-level) evidenceDahm P, Brasure M, MacDonald R, Olson CM, Nelson VA, Fink HA, Rwabasonga B, Risk MC, Wilt TJ. Comparative Effectiveness of Newer Medications for Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: A Systematic Review and Meta-analysis. European urology. 2017 Apr:71(4):570-581. doi: 10.1016/j.eururo.2016.09.032. Epub 2016 Oct 4 [PubMed PMID: 27717522]
Level 2 (mid-level) evidenceKim GE, Kass DA. Cardiac Phosphodiesterases and Their Modulation for Treating Heart Disease. Handbook of experimental pharmacology. 2017:243():249-269. doi: 10.1007/164_2016_82. Epub [PubMed PMID: 27787716]
Redfield MM, Chen HH, Borlaug BA, Semigran MJ, Lee KL, Lewis G, LeWinter MM, Rouleau JL, Bull DA, Mann DL, Deswal A, Stevenson LW, Givertz MM, Ofili EO, O'Connor CM, Felker GM, Goldsmith SR, Bart BA, McNulty SE, Ibarra JC, Lin G, Oh JK, Patel MR, Kim RJ, Tracy RP, Velazquez EJ, Anstrom KJ, Hernandez AF, Mascette AM, Braunwald E, RELAX Trial. Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA. 2013 Mar 27:309(12):1268-77. doi: 10.1001/jama.2013.2024. Epub [PubMed PMID: 23478662]
Level 1 (high-level) evidenceZhang RL, Zhang ZG, Chopp M. Targeting nitric oxide in the subacute restorative treatment of ischemic stroke. Expert opinion on investigational drugs. 2013 Jul:22(7):843-51. doi: 10.1517/13543784.2013.793672. Epub 2013 Apr 18 [PubMed PMID: 23597052]
Level 3 (low-level) evidencePauls MM, Moynihan B, Barrick TR, Kruuse C, Madigan JB, Hainsworth AH, Isaacs JD. The effect of phosphodiesterase-5 inhibitors on cerebral blood flow in humans: A systematic review. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2018 Feb:38(2):189-203. doi: 10.1177/0271678X17747177. Epub 2017 Dec 19 [PubMed PMID: 29256324]
Level 1 (high-level) evidenceTan P, Liu L, Wei S, Tang Z, Yang L, Wei Q. The Effect of Oral Phosphodiesterase-5 Inhibitors on Sperm Parameters: A Meta-analysis and Systematic Review. Urology. 2017 Jul:105():54-61. doi: 10.1016/j.urology.2017.02.032. Epub 2017 Mar 1 [PubMed PMID: 28259808]
Level 1 (high-level) evidenceMónica FZ, De Nucci G. Tadalafil for the treatment of benign prostatic hyperplasia. Expert opinion on pharmacotherapy. 2019 Jun:20(8):929-937. doi: 10.1080/14656566.2019.1589452. Epub 2019 Mar 22 [PubMed PMID: 30901259]
Level 3 (low-level) evidenceGong B, Ma M, Xie W, Yang X, Huang Y, Sun T, Luo Y, Huang J. Direct comparison of tadalafil with sildenafil for the treatment of erectile dysfunction: a systematic review and meta-analysis. International urology and nephrology. 2017 Oct:49(10):1731-1740. doi: 10.1007/s11255-017-1644-5. Epub 2017 Jul 24 [PubMed PMID: 28741090]
Level 1 (high-level) evidenceHuang SA, Lie JD. Phosphodiesterase-5 (PDE5) Inhibitors In the Management of Erectile Dysfunction. P & T : a peer-reviewed journal for formulary management. 2013 Jul:38(7):407-19 [PubMed PMID: 24049429]
Rezaee ME, Gross MS. Are We Overstating the Risk of Priapism With Oral Phosphodiesterase Type 5 Inhibitors? The journal of sexual medicine. 2020 Aug:17(8):1579-1582. doi: 10.1016/j.jsxm.2020.05.019. Epub 2020 Jul 2 [PubMed PMID: 32622767]
Li WQ, Qureshi AA, Robinson KC, Han J. Sildenafil use and increased risk of incident melanoma in US men: a prospective cohort study. JAMA internal medicine. 2014 Jun:174(6):964-70. doi: 10.1001/jamainternmed.2014.594. Epub [PubMed PMID: 24710960]
Carson CC 3rd. Cardiac safety in clinical trials of phosphodiesterase 5 inhibitors. The American journal of cardiology. 2005 Dec 26:96(12B):37M-41M [PubMed PMID: 16387565]
Rosas SE, Joffe M, Franklin E, Strom BL, Kotzker W, Brensinger C, Grossman E, Glasser D, Feldman HI. Prevalence and determinants of erectile dysfunction in hemodialysis patients. Kidney international. 2001 Jun:59(6):2259-66 [PubMed PMID: 11380829]
Level 2 (mid-level) evidenceYafi FA,Sharlip ID,Becher EF, Update on the Safety of Phosphodiesterase Type 5 Inhibitors for the Treatment of Erectile Dysfunction. Sexual medicine reviews. 2018 Apr; [PubMed PMID: 28923561]
Gilad R, Lampl Y, Eshel Y, Sadeh M. Tonic-clonic seizures in patients taking sildenafil. BMJ (Clinical research ed.). 2002 Oct 19:325(7369):869 [PubMed PMID: 12386039]
Level 3 (low-level) evidenceMcLeod AL, McKenna CJ, Northridge DB. Myocardial infarction following the combined recreational use of Viagra and cannabis. Clinical cardiology. 2002 Mar:25(3):133-4 [PubMed PMID: 11890373]
Level 3 (low-level) evidenceBertero E, Montorsi F. Safety of sildenafil citrate: review of 67 double-blind placebo-controlled trials and the postmarketing safety database: F. Giuliano, G. Jackson, F. Montorsi, A. Martin-morales, and P. Raillard. The journal of sexual medicine. 2014 Apr:11(4):885-887. doi: 10.1111/jsm.12513. Epub [PubMed PMID: 24697856]
Level 1 (high-level) evidenceScaglione F, Donde S, Hassan TA, Jannini EA. Phosphodiesterase Type 5 Inhibitors for the Treatment of Erectile Dysfunction: Pharmacology and Clinical Impact of the Sildenafil Citrate Orodispersible Tablet Formulation. Clinical therapeutics. 2017 Feb:39(2):370-377. doi: 10.1016/j.clinthera.2017.01.001. Epub 2017 Jan 28 [PubMed PMID: 28139291]