Introduction
A brain abscess is a localized area of necrosis within the brain parenchyma, typically enclosed by a membrane and most often caused by infections. However, brain abscesses can occasionally result from trauma or surgery.[1][2][3] Although brain abscesses often arise from local infections in areas such as the ear, teeth, sinuses, mastoid air cells, or epidural spaces, they may also originate from distant sites such as the lungs or heart. In young children, brain abscesses may be associated with congenital heart disease. While brain abscesses can occur at any age, they are more prevalent in individuals in their third decade of life.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Brain abscesses can originate locally and spread to other parts of the body. They often form from infections in nearby areas, such as the ear or sinuses, and may occasionally extend from more distant sites, such as the lungs or heart.
Direct Local Spread
Infections in the head and neck region can lead to the development of brain abscesses. Otitis media (5%) and mastoiditis are associated with abscesses in the inferior temporal lobe (see Image. Temporal Lobe Abscess) and cerebellum (see Image. Cerebellar Abscess). Paranasal sinus infections account for 30% to 50% of cases, frequently leading to brain abscesses development. Infections from the frontal or ethmoid sinuses may spread to the frontal lobes, while dental infections commonly result in frontal lobe abscesses.[4]
Facial trauma, including trauma from neurosurgical procedures, can lead to necrotic tissue, which may contribute to brain abscess formation. Metal fragments or other foreign bodies left in the brain parenchyma can also act as a nidus for infection.[1][5]
Generalized Septicemia and Hematogenous Spread
Infectious hematogenous seeding of the brain can arise from various conditions, with the lungs being the most common source. Pulmonary infections, including lung abscesses and empyemas, are frequently seen in individuals with bronchiectasis, and cystic fibrosis is a significant contributing factor.[6]
Additional factors contributing to hematogenous brain seeding include pneumonia, pulmonary arteriovenous malformations (PAVMs), and bronchopleural fistulas. In children, cyanotic congenital heart disease accounts for over 60% of brain abscess cases. Other identified causative factors include bacterial endocarditis, ventricular aneurysms, and thrombosis. Skin, pelvic, and intra-abdominal infections are also commonly reported risk factors.[7]
Approximately 10% of patients with PAVMs develop brain abscesses. Bacteremia-related brain abscesses often result in multiple abscesses, primarily located in the middle cerebral artery distribution, typically at the gray-white matter junction. The most commonly isolated microbial pathogens in brain abscesses are staphylococci and streptococci, with Staphylococcus aureus and viridans streptococci being the most prevalent bacterial species.[8]
A meta-analysis of 9699 patients from 123 studies identified the following list of causative pathogens in brain abscesses:
- Streptococcus species
- S pneumoniae
- Viridans streptococci
- Staphylococcus species
- S aureus
- S epidermidis
- Enterococcus species
- Gram-negative enteric bacteria
- Klebsiella pneumoniae
- Escherichia coli
- Proteus species
- Actinomycetales species
- Corynebacterium
- Nocardia
- Actinomyces
- Mycobacterium tuberculosis
- Haemophilus species
- Pseudomonas species
- Peptostreptococcus species
- Bacteroides species
- Fusobacterium species
- Fungi
- Parasites [9]
Epidemiology
Brain abscesses account for approximately 8% of intracranial masses in low-resource countries and 1% to 2% in high-resource countries, with an incidence of about 4 cases per million. The prevalence of brain abscesses is higher in patients with AIDS compared to the general population, contributing to an increase in cases since the onset of the AIDS pandemic.
Approximately 1500 to 2500 cases of brain abscess are diagnosed annually in the United States. The incidence of fungal brain abscesses has increased due to the rising use of broad-spectrum antibiotics and immunosuppressive agents, such as corticosteroids. Prevalence is highest among adult men aged 30 or younger, while pediatric cases are most common in children aged 4 to 7. Neonates represent the third high-risk group for brain abscess development.
Vaccination has contributed to a reduction in the prevalence of brain abscesses in young children. Data indicate that brain abscesses are more common in males than females, with a male-to-female ratio of 2:1 to 3:1. Geographical and seasonal differences have no significant impact on prevalence. Additionally, brain abscesses account for a disproportionately higher percentage of space-occupying intracranial lesions in low-resource countries.[10][11]
Histopathology
Histological changes in brain abscesses vary based on the stage of infection. In the early stage (within the first 1-2 weeks), known as focal cerebritis, the lesion is poorly demarcated and shows acute inflammatory changes, including vascular congestion and localized cerebral edema. After 2 to 3 weeks, necrosis and liquefaction occur, and the abscess becomes encapsulated by a distinct capsule composed of an inner layer of granulation tissue, a middle collagenous layer, and an outer astroglial layer. The surrounding brain parenchyma is often edematous.
History and Physical
Symptoms are present in about two-thirds of patients for 2 weeks or less, with diagnosis typically established approximately 8 days after symptom onset. The course of the condition can range from indolent to fulminant. Brain abscess manifestations are often nonspecific, which may delay diagnosis. Symptoms largely depend on the size and location of the space-occupying lesion(s). The classic triad of fever, headache, and focal neurologic deficit is observed in fewer than half of patients.
The frequency of common signs and symptoms is as follows:
- Headache (69%-70%) is the most common medical symptom.[9]
- Mental status changes (65%), including lethargy progressing to coma, suggest severe cerebral edema and a poor prognostic sign.
- Focal neurological deficits (50%-65%) typically appear days to weeks after the onset of a headache.
- Pain, usually localized to the location of the abscess, may have a gradual or sudden onset. The pain is often severe and typically not relieved by over-the-counter pain medications.
- Fever (45%-53%)
- Seizures (25%-35%) can be the initial manifestation of a brain abscess, with tonic-clonic seizures being more prevalent in frontal abscesses.
- Nausea and vomiting (40%) are most commonly associated with an occipital lobe abscess or an abscess that has ruptured into a lateral ventricle.
- Nuchal rigidity (15%) is most commonly associated with meningitis or an abscess leaking into a lateral ventricle.
- Cranial nerve deficits involving the third and sixth cranial nerves.
- Rupture of an abscess into a lateral ventricle, which typically presents with a sudden worsening headache, followed by signs of meningismus.
Evaluation
A comprehensive evaluation for a suspected brain abscess involves multiple studies, as listed below.
Laboratory Studies
Routine tests: Routine tests include a complete blood count with differential and platelet count, erythrocyte sedimentation rate, serum C-reactive protein, serological testing, and blood cultures (at least 2, preferably obtained before starting antibiotic therapy).
Lumbar puncture: Rarely required, a lumbar puncture should only be performed after obtaining a head computed tomography (CT) or magnetic resonance imaging (MRI) to rule out increased intracranial pressure due to significant mass effect, which can lead to cerebral herniation and potential mortality. In cases with an acute presentation or suspected meningitis, blood cultures may be used to initiate antibiotic therapy.
Lumbar puncture results are typically nonspecific, showing elevated protein levels, pleocytosis with a variable neutrophil count, normal glucose levels, and sterile cultures. If a rupture occurs in the cerebrospinal fluid (CSF), the white blood cell (WBC) count will increase, and additional findings may include elevated CSF lactic acid levels and abundant red blood cells (RBCs) in the CSF.
Imaging Studies
Imaging studies are crucial for diagnosing and managing brain abscesses, providing essential information on the lesion's size, location, and extent. CT and MRI are the primary modalities used, with MRI offering superior sensitivity for detecting early-stage abscesses and distinguishing them from other intracranial pathologies.
Stereotactic computed tomography or surgical aspiration: Samples can be obtained through surgical aspiration or stereotactic CT-guided aspiration of the abscess. The collected material is sent for diagnostic analysis, including culture, Gram stain, serology, histopathology, and polymerase chain reaction (PCR). These results help guide targeted treatment strategies and monitor the response to therapy, ultimately enhancing overall patient care.
Computed tomography: Although less sensitive than MRI, CT is often used in emergencies.[12] Imaging findings vary based on the stage of the lesion. Early cerebritis typically appears as an irregular, low-density area with no enhancement, though it may show occasional patchy irregular enhancement. As cerebritis progresses, a more defined rim-enhancing lesion becomes visible.
Enzmann et al reported that CT findings of patchy enhancements in early cerebritis evolve into more distinct ring-like enhancements in late cerebritis, eventually forming a frank rim-enhancing brain abscess. A key histopathological difference is that the rim enhancement in late cerebritis lacks the collagen deposition seen in abscesses surrounding a purulent cavity. Serial CT scans obtained in patients with late-stage abscesses demonstrate progressively decreasing edema and mass effect. The abscess wall is typically smooth and regular, measuring 1 to 3 mm thick, and surrounded by parenchymal cerebral edema (see Image. Brain Abscess).
The ring of enhancement may not be uniform in thickness, often appearing relatively thin on the medial or ventricular surface in the deep white matter, where vascularity is less abundant. Steroid administration may reduce edema and contrast enhancement. Multiloculated abscesses with adjacent daughter abscesses or satellite lesions are commonly observed. The presence of gas, if detected, suggests gas-forming organisms.
Magnetic resonance imaging: MRI is the preferred imaging modality for diagnosing and monitoring intracranial lesions due to its heightened sensitivity, particularly in detecting early cerebritis, satellite lesions, and lesions in the brainstem. In addition, MRI allows for a more accurate estimation of necrosis and the full extent of the lesion. MRI provides better differentiation between cerebral edema and brain tissue and is more sensitive in detecting the spread of inflammation into the ventricles and subarachnoid space.[13][14]
Conventional spin-echo imaging with contrast: Classic MRI findings of an abscess include a contrast-enhanced rim surrounding a necrotic core. The rim appears isointense to hyperintense on T1-weighted (T1W) imaging relative to white matter and hypointense on T2-weighted (T2W) imaging. On T2W imaging, the characteristic smooth trilaminar structure of the rim helps distinguish an abscess from other ring-enhancing lesions. Central necrosis shows variable hyperintensity on T2W imaging, depending on the degree of protein content, and appears hypointense on T1W imaging.
Diffusion-weighted magnetic resonance imaging: Diffusion-weighted imaging (DWI) helps differentiate brain abscesses from other ring-enhancing brain lesions. Abscesses typically appear hyperintense on DWI, indicating restricted diffusion, a characteristic feature of viscous materials such as pus. In contrast, neoplasms such as gliomas lack restricted diffusion, appear hypointense, or exhibit variable hyperintensity, which is notably lower than that observed in abscesses.
- Diffusion-tensor imaging: This technique is based on 3-dimensional diffusivity and is commonly used to evaluate white matter tracts. Fractional anisotropy, a quantitative measure derived from diffusion-tensor imaging, assesses the degree of tissue organization. In brain abscesses, fractional anisotropy may be increased, reflecting organized leukocytosis within the abscess cavity and indicating a degree of tissue organization.
- Proton magnetic resonance spectroscopy: This technique evaluates tissue metabolism, with spectral analysis revealing elevated succinate levels, which, although rare, are highly specific for abscesses. Other significant metabolites include increased acetate, alanine, and lactate signals. Amino acids from neutrophil-driven protein breakdown suggest a pyogenic abscess. MR spectroscopy can further differentiate anaerobic from aerobic metabolism by detecting elevated succinate and acetate peaks, which are characteristic of anaerobic infections due to glycolysis and fermentation. Additionally, lactate peaks are lower in strict anaerobes due to their metabolic consumption of lactate.
Brain Biopsy
Needle aspiration or surgical drainage is generally recommended for most patients to establish a diagnosis and identify the causative pathogen.[15] However, an open or stereotactic brain biopsy may be required to confirm a parasitic or fungal abscess. In certain situations, a biopsy may be delayed or deemed unnecessary, such as:
- The presence of a brain abscess alongside bacteremia, particularly when antibiotic therapy corresponds with blood culture results.
- Strong diagnostic support is based on epidemiological, clinical, serological, and neuroimaging findings, such as in cases of neurocysticercosis or toxoplasmosis.
- Abscesses are located in inaccessible or vital regions of the brain.
- A Glasgow coma score of more than 12 and lesions measuring less than 2.5 cm in diameter.
Treatment / Management
A brain abscess can result in elevated intracranial pressure, leading to significant neurological morbidity and mortality. Management typically involves both medical and surgical approaches. Medical management may be appropriate for small, deep-seated abscesses (<2 cm), cases with coexisting meningitis, or specific scenarios such as multiple lesions. However, a combination of medical and surgical interventions is often preferred.[2]
CT and MRI brain imaging are essential for managing brain abscesses, as they aid in localizing the abscess and provide critical details, such as size and number. Depending on available surgical expertise, abscesses larger than 2 cm are typically considered for aspiration or excision. For multiple abscesses, management usually involves a prolonged course of high-dose antibiotics (4-8 weeks) with or without aspirations, guided by weekly CT scans (see Image. Multiple Brain Abscesses).
The antibiotic regimen should be carefully tailored based on the microorganisms isolated from the blood or abscess. Certain antibiotics, such as first-generation cephalosporins, aminoglycosides, and tetracyclines, are less effective for treating brain abscesses due to their limited ability to cross the blood-brain barrier.
Specific antibiotic regimens according to microorganisms are listed below.
- Gram-positive bacteria, including streptococci: Third-generation cephalosporins (eg, cefotaxime and ceftriaxone) or penicillin G are effective.
- S aureus and S epidermis: These bacteria are usually associated with penetrating brain trauma or neurosurgical procedures and should be treated with vancomycin. Vancomycin is also effective for Clostridium species. Linezolid, trimethoprim-sulfamethoxazole, or daptomycin can be considered in cases of vancomycin resistance.
- Fungal infections: Candida and Cryptococcus must be treated with amphotericin B.
- Aspergillus and Pseudallescheria boydii: Voriconazole is the treatment of choice.
- Toxoplasma gondii infection: This is treated with pyrimethamine and sulfadiazine, which can be combined with highly active antiretroviral therapy (HAART) in cases of HIV.
Steroids may be considered in select cases to reduce mass effects, improve antibiotic penetration, and alleviate cerebral edema.[16] However, their use should be judicious, with careful consideration of potential benefits versus the risks of exacerbating an underlying infection, suppressing the immune response, or delaying wound healing.(A1)
The surgical approach plays a pivotal role in managing brain abscesses, with the choice of procedure depending on the operator's skill and preference. Techniques include ultrasound or CT-guided needle aspiration via the stereotactic method, burr hole drainage, and craniotomy for loculated or multiple abscesses. Intravenous (IV) or intrathecal agents targeting specific microorganisms are often used with surgical therapy.[17](A1)
Differential Diagnosis
Differential diagnoses include a range of conditions, such as:
- Bacterial meningitis
- Brain tumors
- Demyelination
- Epidural or subdural abscess
- Encephalitis
- Fungal or parasitic infestations, including cryptococcosis and cysticercosis
- Mycotic aneurysm
- Septic dural sinus thrombosis
Treatment Planning
Antibiotic treatment for brain abscesses is crucial for eradicating the underlying infection and preventing further complications. The selection of antibiotics is guided by the specific microorganisms isolated from cultures and their capacity to effectively penetrate the blood-brain barrier.
Medical therapies include IV treatments against brain abscesses, as outlined below (see Table. Intravenous Therapy Against Brain Abscesses).[18][19]
Table. Intravenous Therapy Against Brain Abscesses
| Antimicrobial Agents | Dosages | Comments |
| Amikacin | 5 mg/kg, 3 times a day |
|
| Ampicillin | 2 g, 6 times a day | |
| Aztreonam | 2 g, 3-4 times a day |
|
| Cefepime | 2 g, 3 times a day | |
| Cefotaxime | 2 g, 4-6 times a day | |
| Ceftaroline | 600 mg, 3 times a day |
|
| Ceftazidime | 2 g, 3 times a day | |
| Ceftriaxone | 2 g, 2 times a day | |
| Ciprofloxacin | 400 mg, 2 to 3 times a day |
|
| Daptomycin | 6-10 mg/kg once a day |
|
| Gentamicin | 1.7 mg/kg, 3 times a day |
|
| Linezolid | 600 mg, 2 times a day |
|
| Meropenem | 2 g, 3 times a day | |
| Metronidazole | 7.5 mg/kg, 3-4 times a day; maximum dose is 4 g/d | |
| Moxifloxacin | 400 mg, once a day |
|
| Nafcillin | 2 g, 6 times a day | |
| Oxacillin | 2 g, 6 times a day | |
| Penicillin G | 4 million units, 6 times a day | |
| Rifampin | 600 mg, once a day |
|
| Tobramycin | 1.7 mg/kg, 3 times a day |
|
| Trimethoprim-sulfamethoxazole (co-trimoxazole) | 5 mg/kg, 2-3 times a day | |
| Vancomycin | 15-20 mg/kg, 2-3 times a day |
Prognosis
With the advent of newer antimicrobials and advanced imaging techniques such as CT and MRI, the mortality rate for brain abscesses has decreased from 10% to 5%. However, the rupture of a brain abscess often remains a fatal complication. Long-term neurological outcomes following infection depend on early diagnosis and prompt administration of antibiotics.
Complications
Complications that can arise secondary to a brain abscess include:
- Meningitis
- Ventriculitis
- Hydrocephalus
- Increased intracranial pressure
- Brain herniation
- Seizures
- Septicemia
- Neurological deficits
- Thrombosis of intracranial blood vessels
- Death
Deterrence and Patient Education
Patients should be educated on the importance of completing the prescribed course of antibiotics and taking anticonvulsants if necessary. In addition, patients should be advised to seek medical attention promptly if they experience a new onset of fever or symptoms of increased intracranial pressure during treatment.
Pearls and Other Issues
Key facts to keep in mind about brain abscesses are as follows:
- A brain abscess is a localized collection of pus within the brain parenchyma, often resulting from infection.
- Common causes include hematogenous spread from distant infections (eg, lung infections and endocarditis), local infections (eg, otitis media and sinusitis), and posttraumatic or postoperative infections.
- Brain abscesses are more prevalent in low-resource countries and among individuals with immunocompromising conditions, such as HIV/AIDS.
- The highest incidence occurs in adults aged 30 or younger and in young children aged 4 to 7.
- Symptoms include headache, fever, focal neurological deficits, seizures, and changes in mental status.
- The classic triad of fever, headaches, and focal neurological deficits is observed in less than half of patients.
- CT scans reveal a ring-enhancing lesion with surrounding edema.
- MRI is preferred for better sensitivity, particularly in the early stages.
- DWI helps differentiate abscesses from other ring-enhancing lesions by showing restricted diffusion.
- Diagnosis is confirmed through imaging and microbiological analysis of the abscess material obtained via aspiration or biopsy.
- Cultures, Gram stain, serology, and PCR help identify causative agents, commonly Staphylococcus and Streptococcus species.
- Medical management includes antibiotics tailored to the identified pathogens.
- Surgical intervention is indicated for large abscesses greater than 2 cm, those causing significant mass effects, or when a definitive diagnosis is necessary.
- Possible complications include rupture into the ventricular system, which can lead to meningitis and worsening of symptoms.
Enhancing Healthcare Team Outcomes
Brain abscesses caused by bacterial infections continue to pose a serious threat to the central nervous system despite advancements in neuroimaging, neurosurgery, improved antibiotics, and modern microbiological techniques.[17] When undiagnosed or untreated, these abscesses can lead to extremely high morbidity and mortality rates. Effective treatment requires an integrated approach involving collaboration among various healthcare professionals.[20]
A recommended interprofessional healthcare team for managing brain abscesses includes:
- Neurosurgeons perform neurosurgical drainage when necessary.
- Radiologists help to locate and evaluate the extent of the abscess.
- Laboratory technologists identify the type of microorganisms growing in the abscess.
- Neurologists monitor patients for neurological deficits.
- Infectious disease specialists determine the source of the infection and recommend appropriate antibiotics.
- Pharmacists manage the choice of antibiotics, address symptoms such as emesis and fever, and assess potential drug-drug interactions.
- Intensivists monitor neurological vital signs in an intensive care unit setting.
- Internists oversee patients with comorbidities such as HIV, immunosuppression, and syndrome of inappropriate secretion of antidiuretic hormone (SIADH).
- Nurses are crucial in monitoring vital signs, administering medications, assessing for gross neurological deficits, and educating families on home management.
All interprofessional healthcare team members should feel empowered to share any findings or evidence of deterioration in the patient's condition, regardless of their discipline. Effective communication within the team is essential, ensuring that all relevant information is conveyed accurately. This collaborative approach enables timely and appropriate therapeutic interventions, ultimately enhancing patient outcomes.
The optimal management of a brain abscess remains a subject of controversy. Current evidence-based medicine lacks conclusive data on key issues, including which patients should be treated with medication alone, the most effective antibiotics with optimal penetrability and efficacy, criteria for surgical intervention, the ideal surgical approach, and long-term outcomes.
To date, randomized clinical trials on the management of brain abscesses are lacking, primarily due to the urgent need for immediate treatment in this medical emergency. Despite the absence of comprehensive data, research studies focused on children with brain abscesses suggest that a combined or interprofessional approach may be the most effective strategy to reduce morbidity and mortality associated with this severe infection.[21]
Media
(Click Image to Enlarge)

Multiple Brain Abscesses. Axial CT scan of the brain with contrast, revealing the presence of multiple abscesses.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)

Temporal Lobe Abscess.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
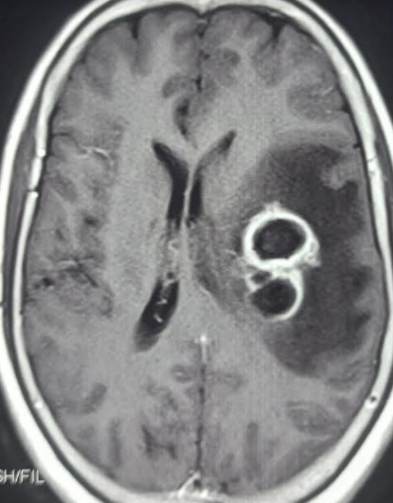
Brain Abscess.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
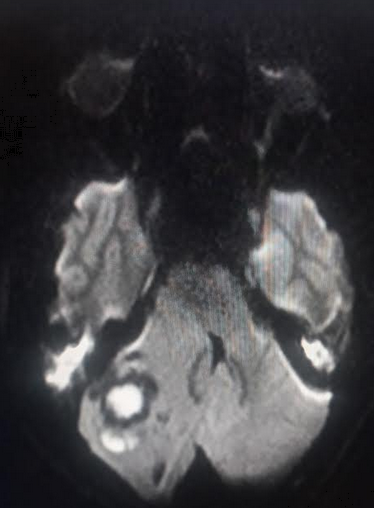
Cerebellar Abscess. Diffusion-weighted MRI image showing a cerebellar abscess displaying the characteristic "light bulb" sign.
Contributed by S Munakomi, MD
References
Lange N, Berndt M, Jörger AK, Wagner A, Wantia N, Lummel N, Ryang YM, Meyer B, Gempt J. Clinical characteristics and course of primary brain abscess. Acta neurochirurgica. 2018 Oct:160(10):2055-2062. doi: 10.1007/s00701-018-3633-6. Epub 2018 Aug 1 [PubMed PMID: 30069602]
Widdrington JD, Bond H, Schwab U, Price DA, Schmid ML, McCarron B, Chadwick DR, Narayanan M, Williams J, Ong E. Pyogenic brain abscess and subdural empyema: presentation, management, and factors predicting outcome. Infection. 2018 Dec:46(6):785-792. doi: 10.1007/s15010-018-1182-9. Epub 2018 Jul 27 [PubMed PMID: 30054798]
Chen M, Low DCY, Low SYY, Muzumdar D, Seow WT. Management of brain abscesses: where are we now? Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2018 Oct:34(10):1871-1880. doi: 10.1007/s00381-018-3886-7. Epub 2018 Jul 3 [PubMed PMID: 29968000]
Salas Olortegui D, Moreno Felici O, Calvó Gómez J, Colomina Rodríguez J. [Eikenella corrodens brain abscess after frontal sinusitis in immunocompetent patient]. Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia. 2023 Apr:36(2):211-213. doi: 10.37201/req/094.2022. Epub 2023 Jan 17 [PubMed PMID: 36648013]
Udayakumaran S, Onyia CU, Kumar RK. Forgotten? Not Yet. Cardiogenic Brain Abscess in Children: A Case Series-Based Review. World neurosurgery. 2017 Nov:107():124-129. doi: 10.1016/j.wneu.2017.07.144. Epub 2017 Aug 2 [PubMed PMID: 28780403]
Level 2 (mid-level) evidenceKapucu I, Kocak M, Kontzialis M. Intracerebral Abscess: An Uncommon Complication of Cystic Fibrosis. The Journal of emergency medicine. 2018 Aug:55(2):e47-e49. doi: 10.1016/j.jemermed.2018.05.017. Epub 2018 Jun 23 [PubMed PMID: 29941375]
Helfritzsch H, Seifert S, Sölch O, Pfister W, Scheele J. [Brain abscess in retroperitoneal perforated colonic diverticulitis]. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen. 2001 Dec:72(12):1427-30 [PubMed PMID: 11824027]
Level 3 (low-level) evidenceNunez FJ, Sharma S, Dahdouh M. Two for the Price of One: A Case of Methicillin-Resistant Staphylococcus aureus (MRSA) Brain Abscess With Atypical Lymphoplasmacytic Infiltrate With Underlying Clonal Lymphoproliferative Process in a Patient Infected With HIV. Cureus. 2023 Jan:15(1):e33325. doi: 10.7759/cureus.33325. Epub 2023 Jan 3 [PubMed PMID: 36741609]
Level 3 (low-level) evidenceBrouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology. 2014 Mar 4:82(9):806-13. doi: 10.1212/WNL.0000000000000172. Epub 2014 Jan 29 [PubMed PMID: 24477107]
Level 1 (high-level) evidenceGorji GRS, Rassouli M, Staji H. Prevalence of cerebral toxoplasmosis among slaughtered sheep in Semnan, Iran. Annals of parasitology. 2018:64(1):37-42. doi: 10.17420/ap6401.130. Epub [PubMed PMID: 29716185]
Maher G, Beniwal M, Bahubali V, Biswas S, Bevinahalli N, Srinivas D, Siddaiah N. Streptococcus pluranimalium: Emerging Animal Streptococcal Species as Causative Agent of Human Brain Abscess. World neurosurgery. 2018 Jul:115():208-212. doi: 10.1016/j.wneu.2018.04.099. Epub 2018 Apr 22 [PubMed PMID: 29689394]
Level 3 (low-level) evidenceShibamura N, Miyamori D, Tanabe T, Yamada N, Tazuma S. Focal Neurological Symptoms at Initial Presentation Could Be a Potential Risk Factor for Poor Prognosis Among Patients With Multiple Brain Abscesses by Streptococcus anginosus Group: A Case Report With Literature Review. Cureus. 2022 Nov:14(11):e32085. doi: 10.7759/cureus.32085. Epub 2022 Nov 30 [PubMed PMID: 36600877]
Level 3 (low-level) evidenceLongo D, Narese D, Fariello G. Diagnosis of brain abscess: a challenge that Magnetic Resonance can help us win! Epidemiology and infection. 2018 Sep:146(12):1608-1610. doi: 10.1017/S0950268818001139. Epub 2018 Jul 4 [PubMed PMID: 29970214]
Berndt M, Lange N, Ryang YM, Meyer B, Zimmer C, Hapfelmeier A, Wantia N, Gempt J, Lummel N. Value of Diffusion-Weighted Imaging in the Diagnosis of Postoperative Intracranial Infections. World neurosurgery. 2018 Oct:118():e245-e253. doi: 10.1016/j.wneu.2018.06.167. Epub 2018 Jun 30 [PubMed PMID: 29966784]
Isern RD 3rd, Toth S, Goldfarb M, Ahmad F. Multifocal Brain Abscesses Due to Streptococcus intermedius. Cureus. 2022 Dec:14(12):e32797. doi: 10.7759/cureus.32797. Epub 2022 Dec 21 [PubMed PMID: 36694540]
Simjian T, Muskens IS, Lamba N, Yunusa I, Wong K, Veronneau R, Kronenburg A, Brouwers HB, Smith TR, Mekary RA, Broekman MLD. Dexamethasone Administration and Mortality in Patients with Brain Abscess: A Systematic Review and Meta-Analysis. World neurosurgery. 2018 Jul:115():257-263. doi: 10.1016/j.wneu.2018.04.130. Epub 2018 Apr 26 [PubMed PMID: 29705232]
Level 1 (high-level) evidenceVieira E, Guimarães TC, Faquini IV, Silva JL, Saboia T, Andrade RVCL, Gemir TL, Neri VC, Almeida NS, Azevedo-Filho HRC. Randomized controlled study comparing 2 surgical techniques for decompressive craniectomy: with watertight duraplasty and without watertight duraplasty. Journal of neurosurgery. 2018 Oct:129(4):1017-1023. doi: 10.3171/2017.4.JNS152954. Epub 2017 Nov 17 [PubMed PMID: 29148904]
Level 1 (high-level) evidenceRybak MJ, Le J, Lodise T, Levine D, Bradley J, Liu C, Mueller B, Pai M, Wong-Beringer A, Rotschafer JC, Rodvold K, Maples HD, Lomaestro BM. Executive Summary: Therapeutic Monitoring of Vancomycin for Serious Methicillin-Resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Journal of the Pediatric Infectious Diseases Society. 2020 Jul 13:9(3):281-284. doi: 10.1093/jpids/piaa057. Epub [PubMed PMID: 32659787]
Level 3 (low-level) evidenceLynch JP 3rd, Zhanel GG. Escalation of antimicrobial resistance among MRSA part 2: focus on infections and treatment. Expert review of anti-infective therapy. 2023 Feb:21(2):115-126. doi: 10.1080/14787210.2023.2154654. Epub 2022 Dec 12 [PubMed PMID: 36469648]
Tunthanathip T, Kanjanapradit K, Sae-Heng S, Oearsakul T, Sakarunchai I. Predictive factors of the outcome and intraventricular rupture of brain abscess. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2015 Feb:98(2):170-80 [PubMed PMID: 25842798]
Capua T, Klivitsky A, Bilavsky E, Ashkenazi-Hoffnung L, Roth J, Constantini S, Grisaru-Soen G. Group A Streptococcal Brain Abscess in the Pediatric Population: Case Series and Review of the Literature. The Pediatric infectious disease journal. 2018 Oct:37(10):967-970. doi: 10.1097/INF.0000000000001947. Epub [PubMed PMID: 29462105]
Level 2 (mid-level) evidence