Definition/Introduction
The Pin Index Safety System (PISS) is a precise configuration of pins and holes that facilitate the connection between a specific medical gas cylinder and its corresponding delivery system.[1] This system was devised to prevent the unintentional placement of a cylinder of the wrong medical gas onto the hanger yoke of the anesthesia machine designed for another gas. Although this system provides an element of safety, it does not eliminate the risk of administering incorrect gas (see Image. Pin Index Safety System).[2]
System Overview
Medical gases for anesthesia machines or workstations are typically supplied through a pipeline from a central piping system. The most commonly used gases include oxygen, medical air, and nitrous oxide. However, when gas supplied through the pipeline is contaminated, fails, or is unavailable, cylinders containing medical gas may be used as an alternative source. The hanger yoke assembly of the anesthesia machine provides orientation and support for the cylinder. Unidirectional airflow and an effective seal are also set by the hanger yoke, and without appropriately placed pins on both the cylinder and yoke, an appropriate seal is not achieved. A special washer or gasket [1] is used to attain this seal, as described below. This system is often utilized for E-cylinders or smaller sizes [3] and is specific for the high-pressure systems within the machine.
History
The first anesthetic machine, known as the Boyle apparatus, was introduced in 1917; however, the PISS was not implemented until the 1950s. Before the use of the PISS, gases were differentiated from each other by the colors of the cylinders and tubing. To prevent the incorrect tubing from being connected to the wrong cylinder—either due to human error or the fading of critical color markings on older tubing—the Ministry of Health in Great Britain [3] introduced the PISS to minimize patient accidents.
Major organizations, such as the American Society of Anesthesiologists, became aware of the vulnerabilities in medical gas delivery systems during World War II. The increased surgeries during the war emphasized the necessity for enhanced anesthetic and surgical safety.[4] As a result, the PISS was introduced, allowing gas cylinders to be equipped with non-interchangeable pin index valves that are specific to the cylinder of a particular medical gas. This system was meant to reduce the probability of a medical gas cylinder being improperly connected to the delivery system. The decision was made to install this system because it could be easily integrated into the machines without requiring a complete overhaul by the manufacturers; instead, it could be fitted by modifying the existing hardware, thereby reducing cost and streamlining implementation. Although it had previously been considered a foolproof safety mechanism, failures of the system have led to quality control improvements and improved safety measures.
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Pin Index Configurations for Commonly Used Medical Gases
Each PISS has 6 possible pin placement sites, depending on the gas within the cylinder. The pins protrude from the gas tank yokes and fit corresponding holes in the cylinder valves, providing a foolproof way to connect the gas to the appropriate valve. Two pins are placed per cylinder, allowing for multiple medically used gases that have been added to the standard formats. The following are examples of pin locations for common medical gases:
- Oxygen: 2, 5
- Nitro oxide: 3, 5
- Air: 1, 5 (see Image. Pin Index Safety System)
- Carbon dioxide: 1, 6
- Nitrogen: 1, 4
These numbers describe the location of the pins in millimeters from the edge of the yoke,[3] with pin #1 being the farthest to the right when looking at the system straight on. The first pin is located 30° from horizontal on the gas tank yoke, and each subsequent pin is located 12° further down, creating a semicircle. These numbers and pin placements are standardized across countries.
Improvements of the Pin Index Safety System
Multiple documented cases of failure of the PISS have led to quality improvements in the system. An early flaw was noted by Pauling in 1983 when a patient died after crossing gas pipelines, leading to the intraoperative delivery of 100% nitrous oxide instead of oxygen. In the weeks leading up to the case, a maintenance team in the hospital had stripped the gas line threads to replace valves but did not independently test the gases that could flow through each line after the work was complete.[5] This case highlights the importance of ensuring proper valve/pin placement. Incorrect setup of any valves, including those involved in filling cylinders, can result in system failure.
A second case report in 1995 documented an incident in which a woman undergoing a laparoscopic cholecystectomy sustained an intra-abdominal fire after a trocar caught fire, leading to the ignition of the insufflating gas within the abdomen. Post-incident analysis revealed that the company providing the gas had a policy that canisters with greater than 7% CO2 were to be fitted with a CO2 pin index; however, this particular canister had a green stripe around the top to identify it as having a majority of O2, not CO2. This specific canister in the operating room was 14% CO2 and 86% O2, leading to the operating room fire. This incident highlighted the potential for human error in the PISS and the potential downfalls in labeling cylinders with mixed gases.[2] Subsequently, efforts were made to distinguish O2 from CO2 and improve oversight.
Clinical Significance
In each of the above cases, thorough investigations were conducted to identify the causes and implement preventive measures. Although the PISS was initially designed for smaller cylinders, its success led to adaptations for larger systems, with some countries mandating pin indexing for even larger cylinders. The crossing of pipelines in hospitals has resulted in more oversight by maintenance crews, and the mislabeling of canisters has since been addressed. Although this system has been designed to improve safety, it also relies upon clinical oversight of medical equipment, staff vigilance, and careful monitoring of anesthesia gas delivery to patients.
Nursing, Allied Health, and Interprofessional Team Interventions
Although the PISS is meant to be a foolproof system, instances have occured where the gas-specific pins have been removed, enabling misconnections and possibly unintended administration of improper gases to patients.[6] Therefore, clinicians using equipment with the PISS should always double check the connections to ensure proper gas delivery.
Media
(Click Image to Enlarge)
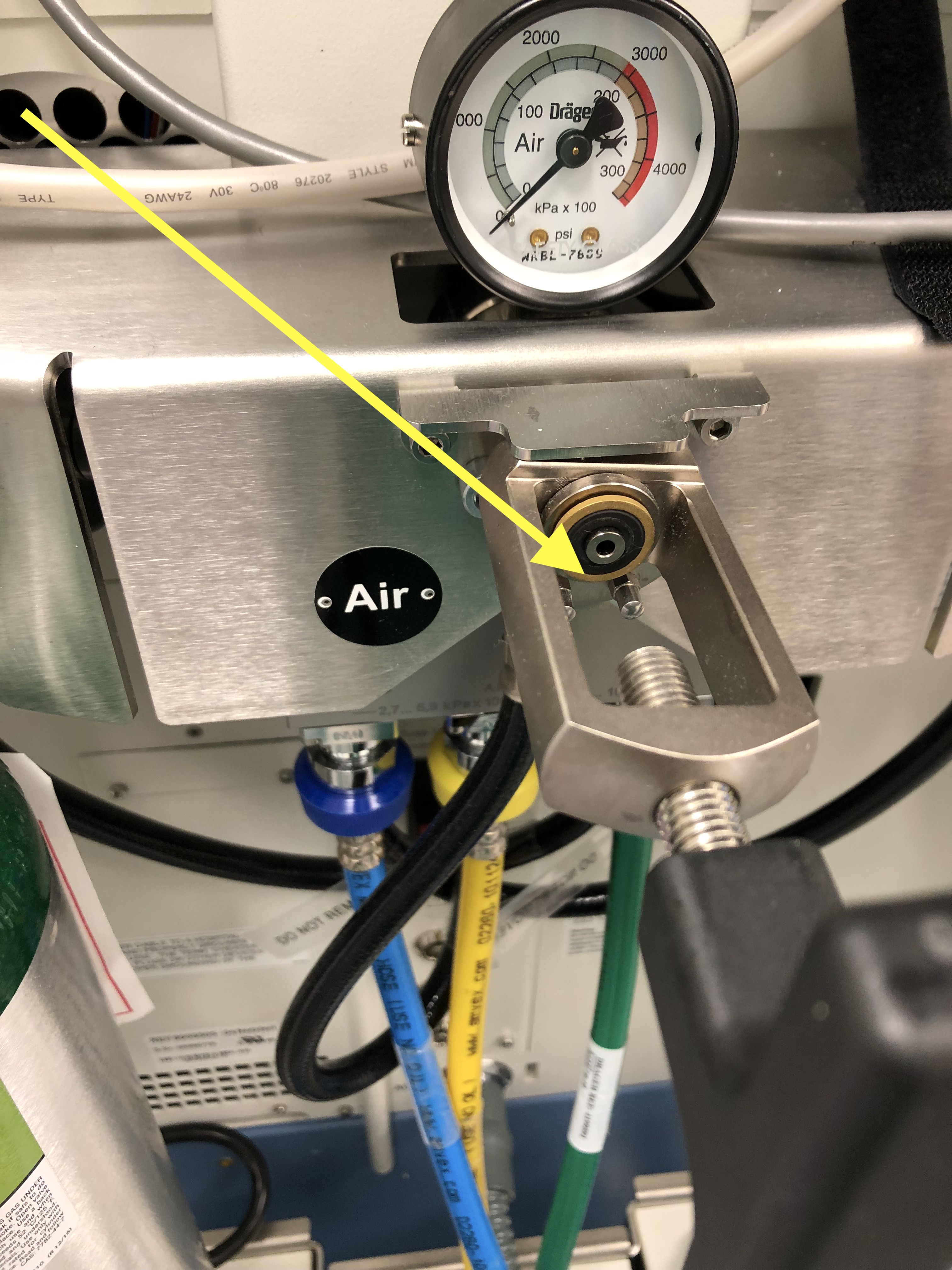
Pin Index Safety System. The image depicts the pins of the hanger yoke intended to secure a cylinder containing medical air. The arrow (yellow) points to the 2 pins, which correspond to pin index configurations 1 and 5. The ring above the 2 pins is visible, where a washer provides a seal to prevent the leakage of medical gas between the gas cylinder and the anesthesia machine/workstation.
Contributed by S Dhanjal, MD
References
Srivastava U. Anaesthesia gas supply: gas cylinders. Indian journal of anaesthesia. 2013 Sep:57(5):500-6. doi: 10.4103/0019-5049.120147. Epub [PubMed PMID: 24249883]
Greilich PE, Greilich NB, Froelich EG. Intraabdominal fire during laparoscopic cholecystectomy. Anesthesiology. 1995 Oct:83(4):871-4 [PubMed PMID: 7574071]
Level 3 (low-level) evidenceDonaldson M, Donaldson D, Quarnstrom FC. Nitrous oxide-oxygen administration: when safety features no longer are safe. Journal of the American Dental Association (1939). 2012 Feb:143(2):134-43 [PubMed PMID: 22298554]
Hogg CE. Pin-indexing failures. Anesthesiology. 1973 Jan:38(1):85-7 [PubMed PMID: 4681954]
Pauling M, Ball CM. Delivery of anoxic gas mixtures in anaesthesia: case report and review of the struggle towards safer standards of care. Anaesthesia and intensive care. 2017 Mar:45(7):21-28 [PubMed PMID: 28675797]
Level 3 (low-level) evidenceIshimura T, Ikuta Y, Yamamoto T. Failure of a "foolproof" pin-index medical pipeline system. JA clinical reports. 2016:2(1):20. doi: 10.1186/s40981-016-0044-7. Epub 2016 Aug 8 [PubMed PMID: 29497675]