Introduction
Overall, about 20% of strokes are hemorrhagic, with SAH and Intracerebral hemorrhage (ICH) each accounting for 10%.[1] Subarachnoid space is described as a space between the arachnoid membrane and the pia mater. It consists of the cerebrospinal fluid and the blood vessels that supply different areas of the brain. A subarachnoid hemorrhage (SAH) is defined as the accumulation of blood in the space between the arachnoid membrane and the pia mater around the brain referred to as the subarachnoid space. The etiology of SAH can be either nontraumatic (about 85% are secondary to aneurysm rupture) or traumatic in nature.[2] In this review, we shall discuss the various aspects of nontraumatic SAH. Most nontraumatic causes of SAH (~ 85%) are caused by the rupture of an intracranial aneurysm. The remaining 15-20% of patients presenting with SAH do not have a vascular lesion on the initial digital subtraction angiography.[3] Regardless of the cause, a SAH is often a devastating clinical event with substantial mortality and high morbidity among survivors. Prehospital care is critical and involves triaging the patient with attention to the airway, breathing, and circulation to a hospital with neurocritical/neurosurgical expertise. The classic presentation is often a sudden-onset, severe headache typically described as the "worst headache of my life". Treatments are based on randomized controlled studies and prospective cohort studies. A SAH has a prolonged course of illness and is complicated by various factors not limited to seizures, vasospasm, hydrocephalus, and delayed cerebral ischemia (DCI). [4][5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
As elucidated earlier, about 85% of nontraumatic SAH cases are secondary to aneurysmal rupture. The remaining 15-20% have a diverse cause, and the mechanism of bleeding is often not identified. Determining the precise etiology of the bleeding is very important, as practitioners can tailor treatment to the cause of the bleeding. The most common causes of nontraumatic SAH are mentioned below:
1) Aneurysmal Subarachnoid hemorrhage (aSAH)
- An aneurysmal cause of SAH has similar risk factors associated with aneurysm formation. Hypertension, cigarette smoking, and family history are the most consistently observed risk factors. Other factors include Alcohol, sympathomimetic drugs, and estrogen deficiency.
- Older age (>60 years), posterior circulation location, atherosclerosis, hypertension, and large Intra-arterial aneurysm (IA) size (>5 mm) are contributing factors for an IA to rupture. A family history of IA or SAH, previous history of SAH, or the presence of autosomal dominant polycystic kidney disease increases the risk of IA rupture.[6]
2) Nonaneurysmal Subarachnoid hemorrhage (NASAH)
i) Perimesencephalic nonaneurysmal subarachnoid hemorrhage: It is characterized by a specific pattern of localized blood on CT, normal cerebral angiography, and a benign course of illness.[7] This subtype makes up the majority, up to two-thirds, of patients with NASAH.[3] The CT findings typically include blood isolated to the perimesencephalic cisterns anterior to the brainstem.[8]
ii) Occult aneurysm: A small percentage of cases are not diagnosed in initial angiographic studies but may be identified on repeat angiography and are classified under this group.[9] The reasons are technical or reading errors, small aneurysm size, and obscuration of aneurysm because of vasospasm, hematoma, or thrombosis within the aneurysm.[10]
iii) Vascular malformations: These can be intracranial or spinal in location. Most brain vascular malformations that cause SAH are either arteriovenous malformations (AVM) or dural arteriovenous fistulae.[11][12] They are usually visualized on cerebral angiography. Dural arteriovenous fistulae are the most common type of spinal vascular malformation.[13] Vascular malformation associated with bleeding is usually managed surgically and or with endovascular interventions.
iv) Intracranial arterial dissection: Dissection of an intracranial artery can produce SAH. When the dissection of the intracranial artery extends through the adventitia, SAH occurs.[14] In these situations, the bleeding is massive and often devastating. This condition is diagnosed by conventional angiography and treated surgically or with endovascular interventions.[14][15][14]
v) Other causes: Cocaine abuse is associated with aneurysmal and nonaneurysmal SAH.[11][16][11] Cerebral amyloid angiopathy can cause SAH in older adults.[17] Cerebral venous thrombosis, sickle cell disorders, moyamoya disease, cerebral vasculitis, and bleeding disorders are some of the conditions that cause SAH.[18][19][20]
Epidemiology
The overall global incidence of aneurysmal SAH was 7.9 per 100,000 person-years.[21] By time trends, in 2010 the incidence of SAH was 6.1 per 100,000 person-years, declining from 1980 when the reported incidence was 10.2 per 100,000 person-years. Around the world, Japan and Finland have higher cases of subarachnoid hemorrhage for reasons unknown.[21]
Most aSAH occur between 40 and 60 years of age, and young children and older adults can be affected.[22] The mean age of aneurysmal rupture ranges from 50-55 years.[23] It is more prevalent in the Blacks and Hispanic populations than the white Americans.[22] There is a slightly higher incidence of aneurysmal SAH in females, which may be related to their hormonal status.[23] Patients with a history of smoking and previously ruptured intracerebral aneurysm are highly associated with new subarachnoid hemorrhage.
Pathophysiology
Hemodynamic stress is the initiating factor for intracranial aneurysm (IA) formation. The observation best illustrates that IAs occur at arterial junctions, bifurcations, or abrupt vascular angles where excessive hemodynamic stresses are exerted on arterial walls.[24] The typical locations include the bifurcation of the basilar artery at the junction of the ipsilateral posterior inferior cerebellar artery (PICA), vertebral artery, and the anterior communicating artery.[25] Large unruptured aneurysms compress the adjacent cerebral tissue causing neurological signs. However, the rupture of these lesions creates a state of reduced blood flow and vasospasm leading to cerebral ischemia. The pathophysiological mechanisms by which these lesions are formed and eventually rupture are not fully understood. The hemodynamic stress to the vessel wall caused by increased blood pressure and other risk factors promotes the formation and rupture of IA.[26] Multiple studies point to inflammation as a dominant factor in the pathogenesis of IA.[27] A hemodynamic insult initiates the inflammatory process. It leads to matrix metalloproteinases (MMPs)–mediated degradation of the extracellular matrix and apoptosis of smooth muscle cells (SMCs), which are the predominant matrix-synthesizing cells of the vascular wall. These processes significantly weaken the arterial wall, resulting in dilatation, aneurysm formation, and ultimately rupture (Figure; Table 1). Notably, The two main constituents of the inflammatory response and the associated degenerative response are macrophages and SMCs.[27]
Histopathology
Aneurysms are divided according to their morphology into:
i) Saccular aneurysms that are pouch-like protrusions of the vessel wall, usually arising in cerebral artery bifurcations (A);
ii) Fusiform aneurysms that are dilatations of the vessel wall that do not lead to the formation of a separate saccular pouch (B); and
iii) dolichoectasias are elongated, tortuous, and sometimes dilated vessel segments (C).
Furthermore, a rare fourth type of cerebral artery aneurysm is the dissecting aneurysm that usually has a fusiform shape (B), but originates from acute dissection or tearing of the arterial wall layers.
History and Physical
A typical presenting symptom is a thunderclap headache. Patients usually describe it as the "worst headache of my life." This problem should prompt further imaging. A headache is frequently associated with nausea, vomiting (often projectile), nuchal rigidity, and photophobia. Meningismus is typically present due to blood extending into the fourth ventricle. As the blood moves further down the spinal cord, it irritates surrounding nerves causing neck pain and stiffness. Practitioners should perform a detailed exam. The presence of a focal deficit increases the grade of subarachnoid hemorrhage and changes the perspective of post-event recovery. Patients with a high-grade subarachnoid hemorrhage often present in a state of coma that calls for an urgent evaluation and treatment, as in some the coma can be reversible.[28] The presence of an unruptured IA or increased intracranial pressure (ICP) post rupture may cause cranial nerve palsies from compression on the third and or sixth cranial nerve (CN III, CN VI).[28] Some patients also experience seizures with IA rupture.[29]
Evaluation
Initial evaluation of a patient suspected of having a subarachnoid hemorrhage should include a head computed tomogram (CT).[30] A CT angiography should be performed if an aSAH is identified to determine the location and size of the aneurysm. However, if the initial Head CT is negative, a lumbar puncture is performed in case of strong suspicion. A lumbar puncture should ideally be performed 6 hours after the initial Head CT to detect the presence of xanthochromia. Often xanthochromia can be assessed at the bedside due to visible cerebrospinal fluid color change.[31] A CT angiogram helps confirm and identify an intracerebral aneurysm's location. If the CT angiogram is negative, it should be followed by cerebral angiography or digital subtraction angiography (DSA).[32] A few factors should be considered in patients allergic to contrast or who have decreased renal function. These patient populations need pre-procedure treatment to decrease the risk of an adverse reaction. Time-of-flight magnetic resonance angiography (TOF-MRA) is another acceptable mode of imaging that does not require contrast injection.[32][33][34]
The sensitivity of CT scans and red blood cell (RBC) counts are time-dependent and very sensitive early in the diagnosis. This loss of sensitivity over time can be due to the brisk physiologic flow of cerebrospinal fluid (CSF). Over time, the RBCs present in the CSF undergo lysis resulting in breakdown products such as bilirubin and oxyhemoglobin. RBC lysis explains that xanthochromia becomes increasingly sensitive after a few hours.
Treatment / Management
All Patients presenting with aSAH should be organized according to the severity of disease. In general, management include medical measures and interventional options like endovascular coiling or direct surgical clipping of the IA. Patients are typically treated with both medical and interventional options. More conservative or less invasive interventions may be sufficient for patients with grade I or II SAH. The key goals for all SAH patients are the prevention of rebleeding, delayed cerebral ischemia (DCI), supportive care, pain management, and accurate diagnosis and treatment.
Although immediate care aims to prevent rebleeding and to secure the aneurysm, other common problems include hydrocephalus and vasospasm. Hydrocephalus is present in up to 30% of patients with intraventricular hemorrhage.[35] The proposed mechanism is thought to be secondary to the mechanical blockage of the CSF flow at different levels and an inflammatory reaction due to the presence of blood in the CSF. This inflammatory reaction eventually leads to the fibrosis of arachnoid granulations.[35] In patients with a significant SAH and a higher (more severe) clinical grade, the incidence of rebleeding is higher and may be evident upon admission to the ED or intensive care unit (ICU). Hydrocephalus often occurs within the first three days post hemorrhage. At this time, placement of an intraventricular external drainage device is recommended to relieve the elevated ICP.[36] Another major complication in aSAH is delayed cerebral ischemia (DCI) development. Approximately 60% of patients with aSAH have radiographic vasospasm, defined as vasoconstriction and narrowing of the cerebral arteries, evident with cerebral angiography with or without clinical signs or symptoms.[37] About 39% of patients will have clinical manifestations of vasospasm. These segments of vasospasm cause reduced blood flow to the brain, causing DCI.(A1)
Osmotic diuretics (i.e., Mannitol) and antihypertensive medications for blood pressure control are required to stabilize the patient until surgical or endovascular interventions can be initiated to secure the IA.[36] Grades III, IV, or V require more aggressive and extensive care that may include intubation and mechanical ventilation to protect the airway and support respiratory effort in patients with decreased levels of consciousness. It is often recommended to place an arterial line for close monitoring of blood pressure. Other interventions may include an indwelling urinary catheter and seizure prophylaxis.[36](A1)
Monitoring
Transcranial Doppler – Transcranial Doppler (TCD) sonography is used for detecting and monitoring vasospasm in SAH. A TCD is able to detect changes in velocity prior to the clinical sequelae of vasospasm. However, it is an operator-dependent technology that has imperfect sensitivity and specificity.[38][39][40][41][38] In general, digital subtraction angiography is required to diagnose vasospasm and institute treatment.(B3)
Imaging studies – In the acute phase of SAH, imaging studies like CT angiography (CTA) and CT perfusion can detect arterial narrowing or perfusion asymmetry. These methods are sensitive and help in predicting delayed cerebral ischemia.[42][43] The use of this technique as a monitoring tool may be limited by risks of recurrent dye loads and radiation exposure.[39] A finding of perfusion-diffusion mismatch on magnetic resonance imaging may be another method of detecting brain areas at risk of infarction in this setting.[44] The clinical utility of either of these methods remains to be established. (B3)
Electroencephalography (EEG) – Continuous EEG can be useful to detect subclinical seizures or nonconvulsive status epilepticus, particularly for patients with poor-grade SAH who develop unexplained neurologic deterioration or fail to improve.[40](B3)
Frequency of neuro checks – Patients with acute SAH should be carefully examined every one to two hours, especially during the high-risk period for delayed cerebral ischemia.[45] Symptomatic vasospasm and delayed cerebral ischemia are manifested clinically by neurologic decline, including the onset of focal neurologic abnormalities.
A development of neurologic deficits should be evaluated with an urgent head CT scan (to identify rebleeding, cerebral infarction, hydrocephalus), angiography (to identify symptomatic vasospasm), and/or EEG (to detect subclinical seizures). Medical complications can also contribute to a change in neurologic status.
Even in the absence of clinical change, it is important to identify cerebral vasospasm and decreased cerebral perfusion. Therefore, some centers monitor all patients with aneurysmal SAH with TCD sonography daily and head CT, CTA, and CT perfusion on admission and between days 3 to 5 and days 7 to 10 to screen for evidence of decreased cerebral perfusion or vasospasm.[45] Digital subtraction angiography can be used in place of CTA/CTP in situations of high suspicion. Additional monitoring may be employed for high-risk patients with poor neurologic status, including EEG, and invasive monitoring of brain tissue oxygenation and cerebral blood flow.[46]
Intracranial pressure monitoring – It is recommended to perform a ventriculostomy in patients with enlarged ventricles on CT or with WFNS scale score ≥3; this allows direct measurement of ICP and also allows treatment by drainage of cerebrospinal fluid (CSF) when appropriate.[47]
Medical Management
The significant concerns after an aSAH are rebleeding, hydrocephalus, and vasospasm. The most immediate problem is rebleeding. The most significant risk of rebleeding and mortality is within the first 6 hours of the initial hemorrhage.[48] Commonly, patients risk rebleeding with elevated systolic blood pressure, poor Hunt-Hess grades, intracerebral or intraventricular hematomas, aneurysms > 10 mm in size, and aneurysms in the posterior circulation.[48]] About 9% to 17% of patients risk rebleeding in the first 72 hours. Rebleeding carries a mortality rate of up to 50%. Nearly 15% of patients rebleed in the first few hours after the initial hemorrhage; however, once the IA is secured, the risk of rebleeding is about 1%.[49] Blood pressure control is a significant component in the prevention of rebleeding.[49] The following section discusses drug therapy used for aSAH, including blood pressure control, vasospasm, and anticoagulants.(A1)
Drug Therapy
Historically, tertiary and academic medical centers have had specialized neuroscience units. In recent years, smaller community hospitals that previously cared for neuroscience patients in general medical or surgical ICUs are becoming specialized. With this, the number of neuroscience/neurological ICUs and specialty medical-surgical units are increasing. The role of neuroscience-specialized pharmacists is growing, providing an additional level of expertise to understand the effects of neurological illness or injury, drug interactions, and the impact on the patient.[50] The pharmacist is vital in managing drugs such as antiepileptics, anticoagulants, antibiotics, pain control, and medications that require pharmacy-dosing services. Patients in the ICU often have multiple continuous intravenous infusions for blood pressure control and sedation and pain medication in addition to scheduled medicines for the prevention of seizures, treatment of hyponatremia, or other complications of aSAH.[50] Neuroscience ICUs have evidence-based, drug-specific protocols to reduce medication errors and decrease provider variability. Optimizing drug protocols can increase patient safety and improve outcomes.[50]
Blood Pressure Control
Blood pressure control is critical to reducing the risk of rebleeding until the IA is secured and during the first 24 to 48 hours postoperative period.[49] The sudden surge in central sympathetic stimulation associated with aSAH results in hypertension, and the generally accepted goal is to maintain the systolic blood pressure to less than 160 mm Hg.[51] The risk of rebleeding is highest in the first 24 hours of the initial hemorrhage and carries a mortality rate up to 78%. Opioid pain medications may help to decrease the blood pressure and promote patient comfort; however, administering rapid-acting intravenous (IV) antihypertensive medications given as needed or via continuous infusion work to maintain the blood pressure within ordered parameters.[49] Nitrates and nitroprusside have fallen out of favor as first-line agents for blood pressure control due to the potential for increased ICP and toxic side effects, particularly with prolonged nitroprusside infusions.[52]
Labetalol and hydralazine are often the favored intermittent dosing medications, whereas nicardipine (Cardene) and clevidipine (Cleviprex) are continuous infusions used for blood pressure control.[49] Labetalol is a beta-blocker that may be administered over 2 minutes in doses ranging from 5 to 20 mg IV every 15 minutes.[53] Hydralazine is given in incremental IV doses of 20 to 40 mg every 30 to 60 minutes. The action of hydralazine is also vasodilation, but with a direct effect on arterioles to decrease systemic resistance and reduce blood pressure.[53] The duration of action is more prolonged than labetalol and lasts 1 to 4 hours with a half-life of 2 to 8 hours. Contraindications include coronary artery disease (CAD). The precaution for stroke patients is to avoid a sudden drop in blood pressure related to antihypertensive medications, particularly in ischemic stroke, that may result in a hypoperfusion injury to the brain.(B3)
Nicardipine (Cardene) is given via continuous IV infusion in titrated doses from 5 to 15 mg/hr to maintain the systolic blood pressure of 150 to 160 mm Hg to prevent rebleeding. Some clinicians prefer to maintain a blood pressure of less than 140 mm Hg to prevent rebleeding.[54] (A1)
Clevidipine (Cleviprex) is also a calcium channel blocker with a similar mechanism of action as nicardipine.[55] The onset of action is about 2 to 4 minutes, with a half-life of about 15 minutes. Dosing and titration begin at 1 to 2 mg/hr and repeated every 90 seconds. Clevidipine is in a lipid base without preservatives.(B3)
Vasospasm Prevention and Treatment
The drug categories that prevent and treat vasospasm include calcium channel blockers, magnesium, endothelin antagonists, and statins. These categories are revieNimodipine following sections to describe their current use, if any, in vasospNimodipinement.
Calcium Channel Blockers
Calcium channel blockers (CCBs) reduce cardiac and smooth muscle contraction without an effect on skeletal muscle. The effectiveness of this classification of drugs in the management of aSAH has been a source of many studies over the years. Still, it is considered that CCBs mitigate the abnormal vasoconstriction of cerebral vascular smooth muscle. Oral administration of the dihydropyridine-type calcium channel blocker nimodipine is the only treatment with consistent, high-quality evidence for decreasing DCI and is now standard of care in patients with aSAH. However, these results are advocated by one large trial.[56][57] These early studies showed the role of oral Nimodipine in reducing DCI and improving outcomes without affecting vasospasm.[58] This suggests nimodipine may have an important vessel-independent effect not completely understood. A recent trial (NEWTON [Nimodipine microparticles to enhance recovery while reducing toxicity after subarachnoid hemorrhage] involving administration of intraventricular nimodipine showed no improvements over standard oral administration.[59] Oral nimodipine is given in doses of 60 mg every 4 hours or 30 mg every 2 hours for 21 days. If hypotension is a recurring problem, the recommendation is to administer smaller, more frequent dosing.(A1)
Magnesium
The use of Magnesium sulfate has shown to have mixed results on neuroprotective and its vasodilatation properties—vasodilation results from an inhibition of Voltage-gated calcium channel-mediated smooth muscle contractions. Various spasmogenic agents such as endothelin-1, norepinephrine, angiotensin II, and serotonin are counteracted by magnesium. The Magnesium for Aneurysmal Subarachnoid Hemorrhage (MASH-2) trial was a phase 3, randomized, placebo-controlled trial. A total of 1,204 patients were enrolled. The study concluded with no improvement in outcomes in the intervention group.[60] Additionally, An updated Cochrane meta-analysis of seven prior randomized trials from MASH-2 and those randomized trials that were eligible for inclusion since the MASH-2 trial involved 2,047 patients demonstrated that magnesium was not superior to a placebo in reducing poor outcomes after aSAH. Therefore, magnesium cannot be recommended for routine administration in aSAH.[61] (A1)
Endothelin Antagonists
Endothelin antagonists (ET-A) are another potential treatment under investigation. ET-A receptors mediate vasoconstriction in arterial smooth muscle. Clazosentan is a selective ET-A receptor antagonist that demonstrated a decrease and a reversal in vasospasm after SAH. One study, CONSCIOUS-1 (Clazosentan to Overcome Neurological Ischemia and Infarct Occurring after Subarachnoid Hemorrhage), found a significant dose-dependent effect on vasospasm when evaluated with angiography. The 413 patients in this study were randomized and given placebo or clazosentan within 56 hours and continued on their assigned protocol for up to 14 days.[62] Subsequent studies with clazosentan have reported no benefit with this drug.(B3)
Statins
Research with statin drugs have also demonstrated a lack of efficacy and have shown no benefit in the treatment of vasospasm and neither does it improve short term or long term outcomes in aSAH[63][64]; however, studies are ongoing. To date, the recommendations have been to continue the statin medication if the patient had been taking it prior to the onset of the SAH.[65](A1)
Anticoagulants
As per the 2015 guidelines from the Neurocritical Care Society (NCS) and Society of Critical Care Medicine (SCCM), it is recommended to discontinue all antithrombotic agents and reverse all anticoagulation until the aneurysm is definitively repaired by surgery or coiling.[66] Patients presenting with aSAH on anticoagulant therapy have a worse prognosis and outcomes. Anticoagulants tend to increase the amount of bleeding at the time of rupture, thereby increasing the overall amount of blood in the subarachnoid space, basal cisterns, and the parenchyma.[67] On the other hand, thrombotic complications related to venous thromboembolism (VTE) may be equally as lethal in patients with stroke. An accepted clinical practice is to initiate pharmacological prophylaxis therapy 24 to 48 hours after surgery with unfractionated or a low-molecular-weight heparin. Nurse-driven protocols often support VTE prevention measures intermittent pneumatic compression (IPC) devices on admission to the critical care unit. Additional measures may consist of early mobilization and prevention of dehydration. Stroke units that promote early mobilization have demonstrated lower rates of DVT.[68] (A1)
Pain Control
Pain management is an essential aspect of patient care. With complaints of the “worst headache of my life”, the interprofessional health care team needs to provide interventions to make the patient as comfortable as possible. Nonopioid medications such as acetaminophen (650 mg PO or 1,000 mg IV) are first line medications and be administered every 4 to 6 hours; however, consideration must be given to contraindications, that is, liver diseaase.[69] NSAIDs like aspirin should be avoided until the aneurysm is secured.[40] Opioid medications such as fentanyl (12.5 to 25 mg IV every hour as needed), Dilaudid (0.2 to 4 mg IV every 3 to 4 hours as needed), and morphine sulfate (2 to 4 mg IV every 1 to 2 hours as required) may provide pain relief as well as a degree of sedation and serve to decrease anxiety. Patients response to pain medications must be monitored closely to avoid oversedation and an inability to accurately assess the patients’ neurological status. Pain management is essential but with caution so that worsening in neurological status is not masked.(B3)
Surgical management
Once an aSAH or a ruptured aneurysm is identified, repair with surgical clipping or endovascular coiling is the only effective treatment and should be performed as early as feasible, preferably within 24 hours [39]; some expert centers report a median time to aneurysm repair of 7 hours from admission.[39] Patients in whom aneurysm treatment is not possible or must be delayed may be candidates for antifibrinolytic therapy, but these agents should not be used for more than 72 hours.[45]
Differential Diagnosis
- Bacterial and tuberculous meningitis
- Granulomatous meningitis
- Neurosarcoidosis
- Pseudo-subarachnoid hemorrhage
Staging
Several grading scales are used in clinical practice to standardize the classification of patients with aSAH and to monitor progression and change in condition. These scales are based on the initial clinical neurological examination and the appearance of blood on the initial head CT. These scales include the Glasgow Coma Scale, the Hunt and Hess grading scale, the WFNS scale, the Fisher grading scale, and the modified Fisher grading scale.
I) The Glasgow Coma Scale (GCS), introduced in 1974, is designed as a reliable and objective scale of neurological function in three subscales of level of consciousness, eye-opening, and motor function.[70] The scale ranges from 3 to 15, and points are denoted based on the level of response. A higher score correlates to a better patient's neurological condition. The GCS is commonly used for the initial and ongoing assessment of a patient with possible or confirmed brain injury. It is used to determine neurological deficits and their changes over time.
II) The World Federation of Neurosurgical Societies (WFNS) developed the WFNS grading scale, which describes the clinical presentation of SAH patients. The scale includes consciousness and motor deficits in its scoring system. The WFNS grading system uses a combination of consciousness and motor deficits from the GCS and the presence of focal neurological deficits to grade the severity of SAH.[71] The scale helps predict recovery and response to treatment. For example, elderly patients with a WFNS grade of I to III have the best clinical recovery and seem to benefit from aggressive treatment compared to patients younger than 70 years with a WFNS score of IV or V.
III) The Hunt and Hess grading scale, introduced in 1968, helps to classify the severity of aSAH based on the patient's clinical condition. It is used as a predictor of a patient's prognosis and outcome. A higher score (grade) correlates to a lower survival rate. [72]
IV) The Fisher grading scale is a numerical scale from 0 to 4 that provides insight into the amount of subarachnoid blood on a CT scan. These grading scales correlate to the hemorrhage's severity, the IA's clinical grade, and the vasospasm's incidence after the SAH. In comparison, the modified Fisher grading scale provides more specific descriptions of the amount and location of blood seen on a CT scan.[73]
Prognosis
SAH is associated with a high early mortality rate.[74] A population-based study published in 2017 found that approximately 18 percent of patients with SAH died suddenly before being evaluated in a hospital.[75] Among patients who reach the hospital alive, much of the subsequent early mortality is caused by the common complications of aneurysmal SAH related to initial bleeding, rebleeding, vasospasm and delayed cerebral ischemia, hydrocephalus, increased intracranial pressure, seizures, and cardiac complications.[75]
Long-term complications of SAH include neurocognitive dysfunction, epilepsy, and other focal neurologic deficits. In one registry, more than 10 percent of patients with SAH remained moderately or severely disabled.[76]
Complications
- Seizures
- Vasospasm
- Rebleed
- Hydrocephalus
- Increased intracranial pressure
- Brain herniation
- Cerebral infarction
- Medical complications
- Neurogenic pulmonary edema[77]
- Death
Consultations
A neurosurgical and neurointerventional consult is essential in the early management of this condition. An interprofessional team can help in making early decisions like coiling or clipping of the culprit aneurysm.
Deterrence and Patient Education
A patient with an aneurysm, who is being conservatively managed should be advised on all the complications that can occur if it ruptures.
Any patient and relatives getting admitted with subarachnoid hemorrhage secondary to an aneurysm rupture should be aware of the chance of rebleed and the morbidity and mortality associated with any intervention.
Enhancing Healthcare Team Outcomes
The majority of patients with subarachnoid hemorrhage present to the emergency department. Thus, the emergency department physician and nurse practitioner must know the workup for these patients. Because of its high mortality, an interprofessional team that includes a Neurosurgeon, Interventional radiologist, Neurologist, Intensivist, and Intensive Care Unit nurses is recommended. Unfortunately, despite optimal care, most patients die within 30 days. Even those who survive are left with severe complications that are disabling.[78][79]
Media
(Click Image to Enlarge)
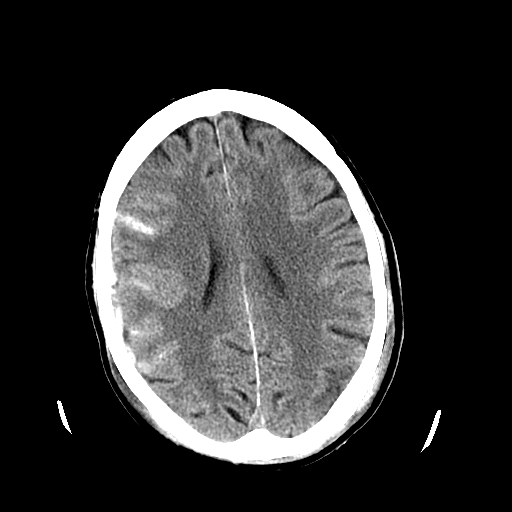
Head CT Revealing Subarachnoid Hemorrhage. The image depicts a head CT scan of a patient revealing a subarachnoid hemorrhage.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
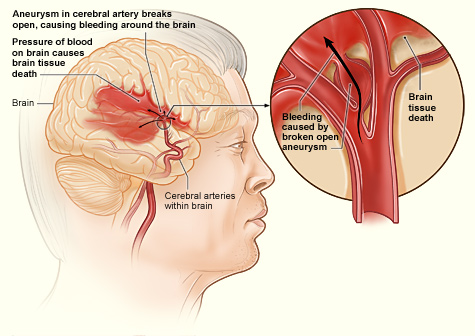
Hemorrhagic Stroke Process. The illustration shows how a hemorrhagic stroke can occur in the brain. An aneurysm in a cerebral artery breaks open, which causes bleeding in the brain. The pressure of the blood causes brain tissue death.
National Heart Lung and Blood Institute
(Click Image to Enlarge)
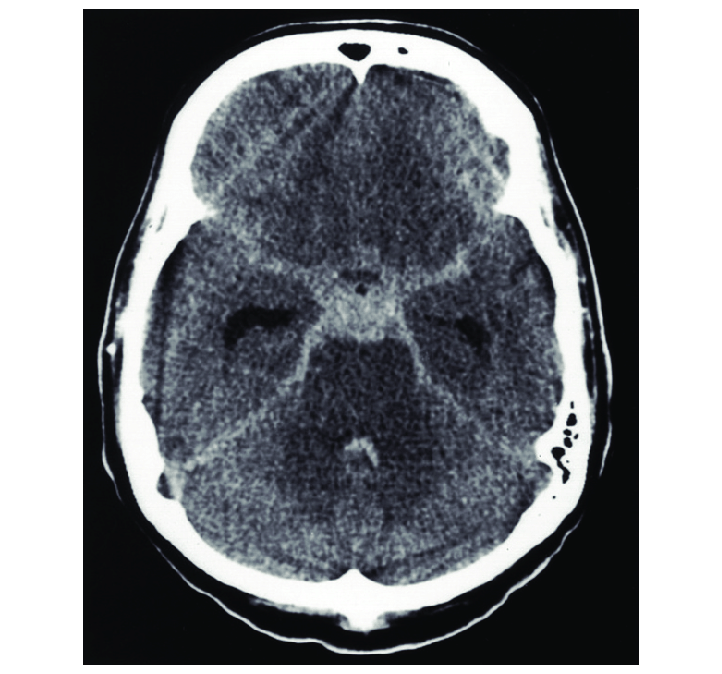
STAR Sign Subarachnoid Hemorrhage
Flynn L, Andrews P. Advances in the understanding of delayed cerebral ischaemia after aneurysmal subarachnoid haemorrhage. F1000Research. 2015;4. doi:10.12688/f1000research.6635.1.
(CC By S.A. 4.0 https://creativecommons.org/licenses/by/4.0)
(Click Image to Enlarge)
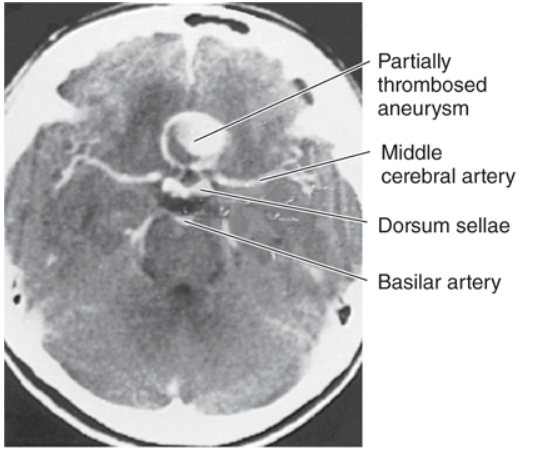
Computed tomography image of a horizontal section through the head, showing a large aneurysm of the anterior communicating artery. (Reproduced with permission from deGroot J: Correlative Neuroanatomy of Computed Tomography and Magnetic Resonance Imaging. Philadelphia, PA: Lea & Febiger; 1984.)
(Click Image to Enlarge)
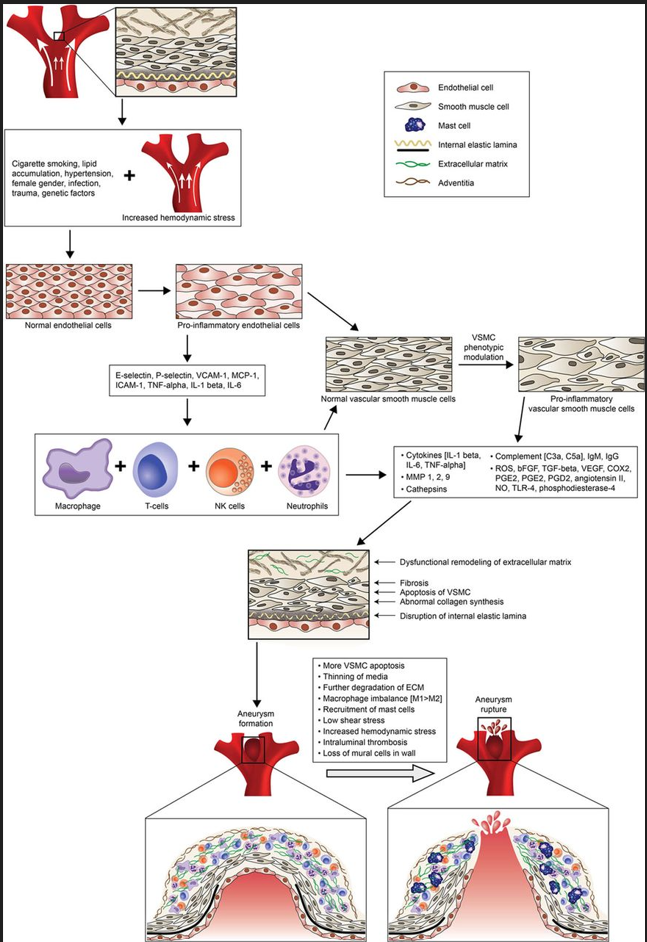
Cerebral aneurysm (CA) formation and rupture. Aneurysm formation is initiated by hemodynamically triggered endothelial dysfunction. An inflammatory response implicating several cytokines and inflammatory mediators as well as macrophages, T cells, and mast cells ensues. Concurrently, smooth muscle cells (SMCs) undergo phenotypic modulation to a proinflammatory phenotype. The inflammatory response in vessel wall leads to disruption of internal elastic lamina, extracellular matrix digestion, and aneurysm formation. Loss of mural cells and further inflammation and vessel wall degeneration ultimately lead to CA rupture. Contributed by Mahammed khan suheb
(Click Image to Enlarge)
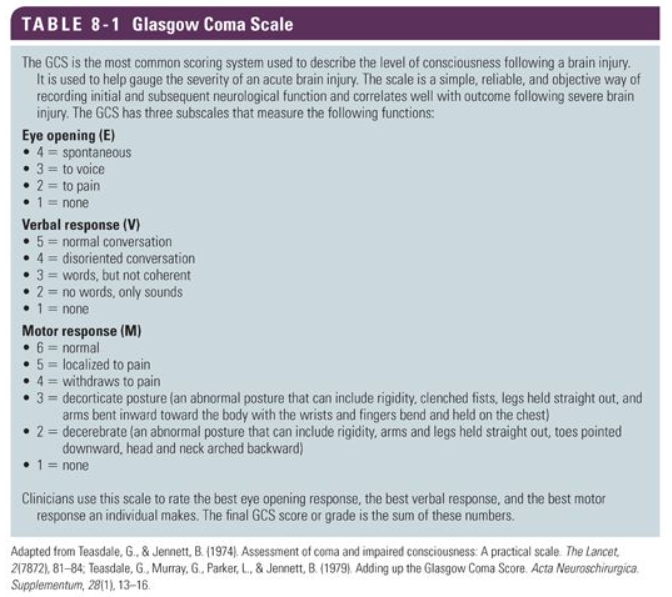
Glasgow coma scale Contributed by Mahammed khan suheb
(Click Image to Enlarge)
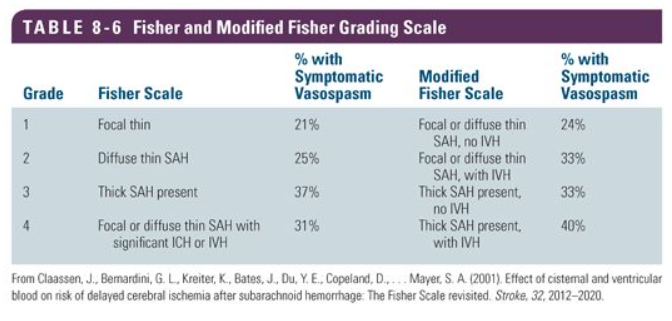
Fischer and modified Fischer scale Contributed by Mahammed khan suheb
(Click Image to Enlarge)
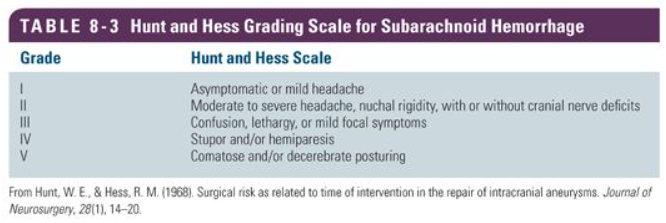
Hunt and Hess scale Contributed by Mahammed khan suheb
(Click Image to Enlarge)
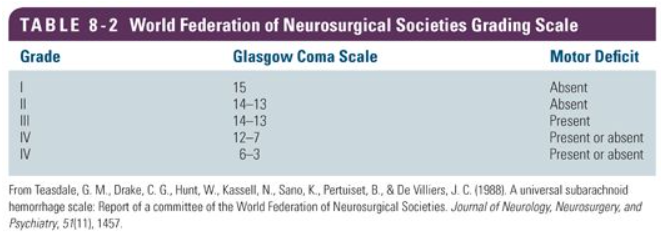
World Federation of Neurological Societies Grading Scale (WFNS) Contributed by Mahammed Khan suheb
References
de Rooij NK, Linn FH, van der Plas JA, Algra A, Rinkel GJ. Incidence of subarachnoid haemorrhage: a systematic review with emphasis on region, age, gender and time trends. Journal of neurology, neurosurgery, and psychiatry. 2007 Dec:78(12):1365-72 [PubMed PMID: 17470467]
Level 1 (high-level) evidenceIkawa F, Michihata N, Matsushige T, Abiko M, Ishii D, Oshita J, Okazaki T, Sakamoto S, Kurogi R, Iihara K, Nishimura K, Morita A, Fushimi K, Yasunaga H, Kurisu K. In-hospital mortality and poor outcome after surgical clipping and endovascular coiling for aneurysmal subarachnoid hemorrhage using nationwide databases: a systematic review and meta-analysis. Neurosurgical review. 2020 Apr:43(2):655-667. doi: 10.1007/s10143-019-01096-2. Epub 2019 Apr 2 [PubMed PMID: 30941595]
Level 1 (high-level) evidenceSchwartz TH, Solomon RA. Perimesencephalic nonaneurysmal subarachnoid hemorrhage: review of the literature. Neurosurgery. 1996 Sep:39(3):433-40; discussion 440 [PubMed PMID: 8875472]
Initial misdiagnosis and outcome after subarachnoid hemorrhage., Kowalski RG,Claassen J,Kreiter KT,Bates JE,Ostapkovich ND,Connolly ES,Mayer SA,, JAMA, 2004 Feb 18 [PubMed PMID: 14970066]
Gallas S,Tuilier T,Ebrahiminia V,Bartoluci P,Hodel J,Gaston A, Intracranial aneurysms in Sickle Cell Disease: Aneurysms characteristics and modalities of endovascular approach to treat these patients. Journal of neuroradiology. Journal de neuroradiologie. 2019 Mar 20; [PubMed PMID: 30904450]
Vlak MH, Rinkel GJ, Greebe P, van der Bom JG, Algra A. Trigger factors for rupture of intracranial aneurysms in relation to patient and aneurysm characteristics. Journal of neurology. 2012 Jul:259(7):1298-302. doi: 10.1007/s00415-011-6341-1. Epub 2011 Dec 21 [PubMed PMID: 22186848]
Level 3 (low-level) evidenceRinkel GJ, Wijdicks EF, Vermeulen M, Ramos LM, Tanghe HL, Hasan D, Meiners LC, van Gijn J. Nonaneurysmal perimesencephalic subarachnoid hemorrhage: CT and MR patterns that differ from aneurysmal rupture. AJNR. American journal of neuroradiology. 1991 Sep-Oct:12(5):829-34 [PubMed PMID: 1950905]
Canhão P, Ferro JM, Pinto AN, Melo TP, Campos JG. Perimesencephalic and nonperimesencephalic subarachnoid haemorrhages with negative angiograms. Acta neurochirurgica. 1995:132(1-3):14-9 [PubMed PMID: 7754850]
Level 2 (mid-level) evidenceTatter SB,Crowell RM,Ogilvy CS, Aneurysmal and microaneurysmal "angiogram-negative" subarachnoid hemorrhage. Neurosurgery. 1995 Jul [PubMed PMID: 8587690]
Level 2 (mid-level) evidenceJung JY, Kim YB, Lee JW, Huh SK, Lee KC. Spontaneous subarachnoid haemorrhage with negative initial angiography: a review of 143 cases. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2006 Dec:13(10):1011-7 [PubMed PMID: 16931020]
Level 2 (mid-level) evidenceRinkel GJ, van Gijn J, Wijdicks EF. Subarachnoid hemorrhage without detectable aneurysm. A review of the causes. Stroke. 1993 Sep:24(9):1403-9 [PubMed PMID: 8362440]
Cordonnier C, Al-Shahi Salman R, Bhattacharya JJ, Counsell CE, Papanastassiou V, Ritchie V, Roberts RC, Sellar RJ, Warlow C, SIVMS Collaborators. Differences between intracranial vascular malformation types in the characteristics of their presenting haemorrhages: prospective, population-based study. Journal of neurology, neurosurgery, and psychiatry. 2008 Jan:79(1):47-51 [PubMed PMID: 17488785]
Koch C. Spinal dural arteriovenous fistula. Current opinion in neurology. 2006 Feb:19(1):69-75 [PubMed PMID: 16415680]
Level 3 (low-level) evidenceCaplan LR. Dissections of brain-supplying arteries. Nature clinical practice. Neurology. 2008 Jan:4(1):34-42. doi: 10.1038/ncpneuro0683. Epub [PubMed PMID: 18199995]
Santos-Franco JA, Zenteno M, Lee A. Dissecting aneurysms of the vertebrobasilar system. A comprehensive review on natural history and treatment options. Neurosurgical review. 2008 Apr:31(2):131-40; discussion 140. doi: 10.1007/s10143-008-0124-x. Epub 2008 Feb 29 [PubMed PMID: 18309525]
Nolte KB, Brass LM, Fletterick CF. Intracranial hemorrhage associated with cocaine abuse: a prospective autopsy study. Neurology. 1996 May:46(5):1291-6 [PubMed PMID: 8628469]
Level 2 (mid-level) evidenceKarabatsou K, Lecky BR, Rainov NG, Broome JC, White RP. Cerebral amyloid angiopathy with symptomatic or occult subarachnoid haemorrhage. European neurology. 2007:57(2):103-5 [PubMed PMID: 17179713]
Level 3 (low-level) evidenceBeitzke M, Gattringer T, Enzinger C, Wagner G, Niederkorn K, Fazekas F. Clinical presentation, etiology, and long-term prognosis in patients with nontraumatic convexal subarachnoid hemorrhage. Stroke. 2011 Nov:42(11):3055-60. doi: 10.1161/STROKEAHA.111.621847. Epub 2011 Sep 15 [PubMed PMID: 21921284]
Level 2 (mid-level) evidenceMarcolini E, Hine J. Approach to the Diagnosis and Management of Subarachnoid Hemorrhage. The western journal of emergency medicine. 2019 Mar:20(2):203-211. doi: 10.5811/westjem.2019.1.37352. Epub 2019 Feb 28 [PubMed PMID: 30881537]
Kuroda H, Mochizuki T, Shimizu S, Kumabe T. Rupture of Thrombosed Cerebral Aneurysm During Antithrombotic Therapy for Ischemic Stroke: Case Report and Literature Review. World neurosurgery. 2019 Jun:126():468-471. doi: 10.1016/j.wneu.2019.02.238. Epub 2019 Mar 18 [PubMed PMID: 30898732]
Level 3 (low-level) evidenceEtminan N, Chang HS, Hackenberg K, de Rooij NK, Vergouwen MDI, Rinkel GJE, Algra A. Worldwide Incidence of Aneurysmal Subarachnoid Hemorrhage According to Region, Time Period, Blood Pressure, and Smoking Prevalence in the Population: A Systematic Review and Meta-analysis. JAMA neurology. 2019 May 1:76(5):588-597. doi: 10.1001/jamaneurol.2019.0006. Epub [PubMed PMID: 30659573]
Level 1 (high-level) evidenceShea AM, Reed SD, Curtis LH, Alexander MJ, Villani JJ, Schulman KA. Characteristics of nontraumatic subarachnoid hemorrhage in the United States in 2003. Neurosurgery. 2007 Dec:61(6):1131-7; discussion 1137-8 [PubMed PMID: 18162891]
Level 2 (mid-level) evidenceRinkel GJ,Djibuti M,Algra A,van Gijn J, Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke. 1998 Jan; [PubMed PMID: 9445359]
Level 2 (mid-level) evidenceChalouhi N, Ali MS, Jabbour PM, Tjoumakaris SI, Gonzalez LF, Rosenwasser RH, Koch WJ, Dumont AS. Biology of intracranial aneurysms: role of inflammation. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2012 Sep:32(9):1659-76. doi: 10.1038/jcbfm.2012.84. Epub 2012 Jul 11 [PubMed PMID: 22781330]
Level 3 (low-level) evidenceBrisman JL, Song JK, Newell DW. Cerebral aneurysms. The New England journal of medicine. 2006 Aug 31:355(9):928-39 [PubMed PMID: 16943405]
Penn DL, Komotar RJ, Sander Connolly E. Hemodynamic mechanisms underlying cerebral aneurysm pathogenesis. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2011 Nov:18(11):1435-8. doi: 10.1016/j.jocn.2011.05.001. Epub 2011 Sep 14 [PubMed PMID: 21917457]
Chalouhi N, Hoh BL, Hasan D. Review of cerebral aneurysm formation, growth, and rupture. Stroke. 2013 Dec:44(12):3613-22. doi: 10.1161/STROKEAHA.113.002390. Epub 2013 Oct 15 [PubMed PMID: 24130141]
Green DM, Burns JD, DeFusco CM. ICU management of aneurysmal subarachnoid hemorrhage. Journal of intensive care medicine. 2013 Nov-Dec:28(6):341-54. doi: 10.1177/0885066611434100. Epub 2012 Feb 11 [PubMed PMID: 22328599]
Level 3 (low-level) evidenceDiringer MN. Management of aneurysmal subarachnoid hemorrhage. Critical care medicine. 2009 Feb:37(2):432-40. doi: 10.1097/CCM.0b013e318195865a. Epub [PubMed PMID: 19114880]
Vermeulen M, van Gijn J. The diagnosis of subarachnoid haemorrhage. Journal of neurology, neurosurgery, and psychiatry. 1990 May:53(5):365-72 [PubMed PMID: 2191083]
Edlow JA. Managing Patients With Nontraumatic, Severe, Rapid-Onset Headache. Annals of emergency medicine. 2018 Mar:71(3):400-408. doi: 10.1016/j.annemergmed.2017.04.044. Epub [PubMed PMID: 28601276]
Kumar A, Niknam K, Lumba-Brown A, Woodruff M, Bledsoe JR, Kohn MA, Perry JJ, Govindarajan P. Practice Variation in the Diagnosis of Aneurysmal Subarachnoid Hemorrhage: A Survey of US and Canadian Emergency Medicine Physicians. Neurocritical care. 2019 Oct:31(2):321-328. doi: 10.1007/s12028-019-00679-7. Epub [PubMed PMID: 30790225]
Level 3 (low-level) evidenceLi K, Barras CD, Chandra RV, Kok HK, Maingard JT, Carter NS, Russell JH, Lai L, Brooks M, Asadi H. A Review of the Management of Cerebral Vasospasm After Aneurysmal Subarachnoid Hemorrhage. World neurosurgery. 2019 Jun:126():513-527. doi: 10.1016/j.wneu.2019.03.083. Epub 2019 Mar 18 [PubMed PMID: 30898740]
Dodson V, Majmundar N, El-Ghanem M, Amuluru K, Gupta G, Nuoman R, Wainwright J, Kaur G, Cole C, Santarelli J, Chandy D, Bowers C, Gandhi C, Al-Mufti F. Intracranial Administration of Nicardipine After Aneurysmal Subarachnoid Hemorrhage: A Review of the Literature. World neurosurgery. 2019 May:125():511-518.e1. doi: 10.1016/j.wneu.2019.01.103. Epub 2019 Jan 29 [PubMed PMID: 30708083]
Chen S, Luo J, Reis C, Manaenko A, Zhang J. Hydrocephalus after Subarachnoid Hemorrhage: Pathophysiology, Diagnosis, and Treatment. BioMed research international. 2017:2017():8584753. doi: 10.1155/2017/8584753. Epub 2017 Mar 8 [PubMed PMID: 28373987]
Bederson JB, Connolly ES Jr, Batjer HH, Dacey RG, Dion JE, Diringer MN, Duldner JE Jr, Harbaugh RE, Patel AB, Rosenwasser RH, American Heart Association. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 2009 Mar:40(3):994-1025. doi: 10.1161/STROKEAHA.108.191395. Epub 2009 Jan 22 [PubMed PMID: 19164800]
Level 1 (high-level) evidenceDodd WS, Laurent D, Dumont AS, Hasan DM, Jabbour PM, Starke RM, Hosaka K, Polifka AJ, Hoh BL, Chalouhi N. Pathophysiology of Delayed Cerebral Ischemia After Subarachnoid Hemorrhage: A Review. Journal of the American Heart Association. 2021 Aug 3:10(15):e021845. doi: 10.1161/JAHA.121.021845. Epub 2021 Jul 30 [PubMed PMID: 34325514]
Djelilovic-Vranic J, Basic-Kes V, Tiric-Campara M, Djozic E, Kulenovic J. Follow-up of Vasospasm by Transcranial Doppler Sonography (TCD) in Subarachnoid Hemorrhage (SAH). Acta informatica medica : AIM : journal of the Society for Medical Informatics of Bosnia & Herzegovina : casopis Drustva za medicinsku informatiku BiH. 2017 Mar:25(1):14-18. doi: 10.5455/aim.2017.25.14-18. Epub [PubMed PMID: 28484291]
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, Hoh BL, Kirkness CJ, Naidech AM, Ogilvy CS, Patel AB, Thompson BG, Vespa P, American Heart Association Stroke Council, Council on Cardiovascular Radiology and Intervention, Council on Cardiovascular Nursing, Council on Cardiovascular Surgery and Anesthesia, Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012 Jun:43(6):1711-37. doi: 10.1161/STR.0b013e3182587839. Epub 2012 May 3 [PubMed PMID: 22556195]
Diringer MN, Bleck TP, Claude Hemphill J 3rd, Menon D, Shutter L, Vespa P, Bruder N, Connolly ES Jr, Citerio G, Gress D, Hänggi D, Hoh BL, Lanzino G, Le Roux P, Rabinstein A, Schmutzhard E, Stocchetti N, Suarez JI, Treggiari M, Tseng MY, Vergouwen MD, Wolf S, Zipfel G, Neurocritical Care Society. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society's Multidisciplinary Consensus Conference. Neurocritical care. 2011 Sep:15(2):211-40. doi: 10.1007/s12028-011-9605-9. Epub [PubMed PMID: 21773873]
Level 3 (low-level) evidenceKrejza J, Kochanowicz J, Mariak Z, Lewko J, Melhem ER. Middle cerebral artery spasm after subarachnoid hemorrhage: detection with transcranial color-coded duplex US. Radiology. 2005 Aug:236(2):621-9 [PubMed PMID: 16040918]
van der Schaaf I, Wermer MJ, van der Graaf Y, Velthuis BK, van de Kraats CI, Rinkel GJ. Prognostic value of cerebral perfusion-computed tomography in the acute stage after subarachnoid hemorrhage for the development of delayed cerebral ischemia. Stroke. 2006 Feb:37(2):409-13 [PubMed PMID: 16373646]
Level 3 (low-level) evidencevan der Schaaf I, Wermer MJ, van der Graaf Y, Hoff RG, Rinkel GJ, Velthuis BK. CT after subarachnoid hemorrhage: relation of cerebral perfusion to delayed cerebral ischemia. Neurology. 2006 May 23:66(10):1533-8 [PubMed PMID: 16717213]
Vatter H, Güresir E, Berkefeld J, Beck J, Raabe A, du Mesnil de Rochemont R, Seifert V, Weidauer S. Perfusion-diffusion mismatch in MRI to indicate endovascular treatment of cerebral vasospasm after subarachnoid haemorrhage. Journal of neurology, neurosurgery, and psychiatry. 2011 Aug:82(8):876-83. doi: 10.1136/jnnp.2010.219592. Epub 2011 Mar 24 [PubMed PMID: 21436228]
Suarez JI. Diagnosis and Management of Subarachnoid Hemorrhage. Continuum (Minneapolis, Minn.). 2015 Oct:21(5 Neurocritical Care):1263-87. doi: 10.1212/CON.0000000000000217. Epub [PubMed PMID: 26426230]
Francoeur CL, Mayer SA. Management of delayed cerebral ischemia after subarachnoid hemorrhage. Critical care (London, England). 2016 Oct 14:20(1):277 [PubMed PMID: 27737684]
Hellingman CA, van den Bergh WM, Beijer IS, van Dijk GW, Algra A, van Gijn J, Rinkel GJ. Risk of rebleeding after treatment of acute hydrocephalus in patients with aneurysmal subarachnoid hemorrhage. Stroke. 2007 Jan:38(1):96-9 [PubMed PMID: 17122426]
Tang C, Zhang TS, Zhou LF. Risk factors for rebleeding of aneurysmal subarachnoid hemorrhage: a meta-analysis. PloS one. 2014:9(6):e99536. doi: 10.1371/journal.pone.0099536. Epub 2014 Jun 9 [PubMed PMID: 24911172]
Level 1 (high-level) evidenceD'Souza S. Aneurysmal Subarachnoid Hemorrhage. Journal of neurosurgical anesthesiology. 2015 Jul:27(3):222-40. doi: 10.1097/ANA.0000000000000130. Epub [PubMed PMID: 25272066]
Rhoney DH. Introduction: neurologic critical care. Journal of pharmacy practice. 2010 Oct:23(5):385-6. doi: 10.1177/0897190010372319. Epub [PubMed PMID: 21507843]
Bath PM, Song L, Silva GS, Mistry E, Petersen N, Tsivgoulis G, Mazighi M, Bang OY, Sandset EC. Blood Pressure Management for Ischemic Stroke in the First 24 Hours. Stroke. 2022 Apr:53(4):1074-1084. doi: 10.1161/STROKEAHA.121.036143. Epub 2022 Mar 16 [PubMed PMID: 35291822]
Osgood ML. Aneurysmal Subarachnoid Hemorrhage: Review of the Pathophysiology and Management Strategies. Current neurology and neuroscience reports. 2021 Jul 26:21(9):50. doi: 10.1007/s11910-021-01136-9. Epub 2021 Jul 26 [PubMed PMID: 34308493]
MacCarthy EP, Bloomfield SS. Labetalol: a review of its pharmacology, pharmacokinetics, clinical uses and adverse effects. Pharmacotherapy. 1983 Jul-Aug:3(4):193-219 [PubMed PMID: 6310529]
Level 3 (low-level) evidenceHuang RQ, Jiang FG, Feng ZM, Wang TY. Nicardipine in the treatment of aneurysmal subarachnoid haemorrhage: a meta-analysis of published data. Acta neurologica Belgica. 2013 Mar:113(1):3-6. doi: 10.1007/s13760-012-0142-x. Epub 2012 Oct 31 [PubMed PMID: 23111775]
Level 1 (high-level) evidenceVarelas PN, Abdelhak T, Corry JJ, James E, Rehman MF, Schultz L, Mays-Wilson K, Mitsias P. Clevidipine for acute hypertension in patients with subarachnoid hemorrhage: a pilot study. The International journal of neuroscience. 2014 Mar:124(3):192-8. doi: 10.3109/00207454.2013.836703. Epub 2013 Sep 24 [PubMed PMID: 24007334]
Level 3 (low-level) evidenceDorhout Mees SM, Rinkel GJ, Feigin VL, Algra A, van den Bergh WM, Vermeulen M, van Gijn J. Calcium antagonists for aneurysmal subarachnoid haemorrhage. The Cochrane database of systematic reviews. 2007 Jul 18:2007(3):CD000277 [PubMed PMID: 17636626]
Level 1 (high-level) evidencePickard JD, Murray GD, Illingworth R, Shaw MD, Teasdale GM, Foy PM, Humphrey PR, Lang DA, Nelson R, Richards P. Effect of oral nimodipine on cerebral infarction and outcome after subarachnoid haemorrhage: British aneurysm nimodipine trial. BMJ (Clinical research ed.). 1989 Mar 11:298(6674):636-42 [PubMed PMID: 2496789]
Level 1 (high-level) evidencePetruk KC, West M, Mohr G, Weir BK, Benoit BG, Gentili F, Disney LB, Khan MI, Grace M, Holness RO. Nimodipine treatment in poor-grade aneurysm patients. Results of a multicenter double-blind placebo-controlled trial. Journal of neurosurgery. 1988 Apr:68(4):505-17 [PubMed PMID: 3280746]
Level 1 (high-level) evidenceCarlson AP, Hänggi D, Wong GK, Etminan N, Mayer SA, Aldrich F, Diringer MN, Schmutzhard E, Faleck HJ, Ng D, Saville BR, Bleck T, Grubb R Jr, Miller M, Suarez JI, Proskin HM, Macdonald RL, NEWTON Investigators. Single-Dose Intraventricular Nimodipine Microparticles Versus Oral Nimodipine for Aneurysmal Subarachnoid Hemorrhage. Stroke. 2020 Apr:51(4):1142-1149. doi: 10.1161/STROKEAHA.119.027396. Epub 2020 Mar 6 [PubMed PMID: 32138631]
Dorhout Mees SM, Algra A, Vandertop WP, van Kooten F, Kuijsten HA, Boiten J, van Oostenbrugge RJ, Al-Shahi Salman R, Lavados PM, Rinkel GJ, van den Bergh WM, MASH-2 Study Group. Magnesium for aneurysmal subarachnoid haemorrhage (MASH-2): a randomised placebo-controlled trial. Lancet (London, England). 2012 Jul 7:380(9836):44-9. doi: 10.1016/S0140-6736(12)60724-7. Epub 2012 May 25 [PubMed PMID: 22633825]
Level 3 (low-level) evidenceDorhout Mees SM, Algra A, Wong GK, Poon WS, Bradford CM, Saver JL, Starkman S, Rinkel GJ, van den Bergh WM, writing groups of MASH-I, IMASH, MASH-II, MASH and FAST-MAG, van Kooten F, Dirven CM, van Gijn J, Vermeulen M, Rinkel GJ, Boet R, Chan MT, Gin T, Ng SC, Zee BC, Al-Shahi Salman R, Boiten J, Kuijsten H, Lavados PM, van Oostenbrugge RJ, Vandertop WP, Finfer S, O'Connor A, Yarad E, Firth R, McCallister R, Harrington T, Steinfort B, Faulder K, Assaad N, Morgan M, Starkman S, Eckstein M, Stratton SJ, Pratt FD, Hamilton S, Conwit R, Liebeskind DS, Sung G, Kramer I, Moreau G, Goldweber R, Sanossian N. Early Magnesium Treatment After Aneurysmal Subarachnoid Hemorrhage: Individual Patient Data Meta-Analysis. Stroke. 2015 Nov:46(11):3190-3. doi: 10.1161/STROKEAHA.115.010575. Epub 2015 Oct 13 [PubMed PMID: 26463689]
Level 1 (high-level) evidenceRhoney DH, McAllen K, Liu-DeRyke X. Current and future treatment considerations in the management of aneurysmal subarachnoid hemorrhage. Journal of pharmacy practice. 2010 Oct:23(5):408-24. doi: 10.1177/0897190010372334. Epub 2010 Aug 12 [PubMed PMID: 21507846]
Level 3 (low-level) evidenceKirkpatrick PJ, Turner CL, Smith C, Hutchinson PJ, Murray GD, STASH Collaborators. Simvastatin in aneurysmal subarachnoid haemorrhage (STASH): a multicentre randomised phase 3 trial. The Lancet. Neurology. 2014 Jul:13(7):666-75. doi: 10.1016/S1474-4422(14)70084-5. Epub 2014 May 15 [PubMed PMID: 24837690]
Level 1 (high-level) evidenceWong GK, Chan DY, Siu DY, Zee BC, Poon WS, Chan MT, Gin T, Leung M, HDS-SAH Investigators. High-dose simvastatin for aneurysmal subarachnoid hemorrhage: multicenter randomized controlled double-blinded clinical trial. Stroke. 2015 Feb:46(2):382-8. doi: 10.1161/STROKEAHA.114.007006. Epub 2014 Dec 16 [PubMed PMID: 25516195]
Level 1 (high-level) evidenceLiu J, Chen Q. Effect of statins treatment for patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis of observational studies and randomized controlled trials. International journal of clinical and experimental medicine. 2015:8(5):7198-208 [PubMed PMID: 26221259]
Level 1 (high-level) evidenceFrontera JA, Lewin JJ 3rd, Rabinstein AA, Aisiku IP, Alexandrov AW, Cook AM, del Zoppo GJ, Kumar MA, Peerschke EI, Stiefel MF, Teitelbaum JS, Wartenberg KE, Zerfoss CL. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocritical care. 2016 Feb:24(1):6-46. doi: 10.1007/s12028-015-0222-x. Epub [PubMed PMID: 26714677]
Rinkel GJ, Prins NE, Algra A. Outcome of aneurysmal subarachnoid hemorrhage in patients on anticoagulant treatment. Stroke. 1997 Jan:28(1):6-9 [PubMed PMID: 8996479]
Xu T, Yu X, Ou S, Liu X, Yuan J, Chen Y. Efficacy and Safety of Very Early Mobilization in Patients with Acute Stroke: A Systematic Review and Meta-analysis. Scientific reports. 2017 Jul 26:7(1):6550. doi: 10.1038/s41598-017-06871-z. Epub 2017 Jul 26 [PubMed PMID: 28747763]
Level 1 (high-level) evidenceMuehlschlegel S. Subarachnoid Hemorrhage. Continuum (Minneapolis, Minn.). 2018 Dec:24(6):1623-1657. doi: 10.1212/CON.0000000000000679. Epub [PubMed PMID: 30516599]
Teasdale G, Murray G, Parker L, Jennett B. Adding up the Glasgow Coma Score. Acta neurochirurgica. Supplementum. 1979:28(1):13-6 [PubMed PMID: 290137]
Teasdale GM, Drake CG, Hunt W, Kassell N, Sano K, Pertuiset B, De Villiers JC. A universal subarachnoid hemorrhage scale: report of a committee of the World Federation of Neurosurgical Societies. Journal of neurology, neurosurgery, and psychiatry. 1988 Nov:51(11):1457 [PubMed PMID: 3236024]
Level 3 (low-level) evidenceHunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. Journal of neurosurgery. 1968 Jan:28(1):14-20 [PubMed PMID: 5635959]
Claassen J, Bernardini GL, Kreiter K, Bates J, Du YE, Copeland D, Connolly ES, Mayer SA. Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after subarachnoid hemorrhage: the Fisher scale revisited. Stroke. 2001 Sep:32(9):2012-20 [PubMed PMID: 11546890]
van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet (London, England). 2007 Jan 27:369(9558):306-18 [PubMed PMID: 17258671]
Lindbohm JV, Kaprio J, Jousilahti P, Salomaa V, Korja M. Risk Factors of Sudden Death From Subarachnoid Hemorrhage. Stroke. 2017 Sep:48(9):2399-2404. doi: 10.1161/STROKEAHA.117.018118. Epub 2017 Jul 24 [PubMed PMID: 28739833]
Schatlo B,Fung C,Stienen MN,Fathi AR,Fandino J,Smoll NR,Zumofen D,Daniel RT,Burkhardt JK,Bervini D,Marbacher S,Reinert M,D Alonzo D,Ahlborn P,Mendes Pereira V,Roethlisberger M,Seule M,Kerkeni H,Remonda L,Weyerbrock A,Woernle K,Venier A,Perren F,Sailer M,Robert T,Rohde V,Schöni D,Goldberg J,Nevzati E,Diepers M,Gralla J,Z'Graggen W,Starnoni D,Woernle C,Maldaner N,Kulcsar Z,Mostaguir K,Maduri R,Eisenring C,Bernays R,Ferrari A,Dan-Ura H,Finkenstädt S,Gasche Y,Sarrafzadeh A,Jakob SM,Corniola M,Baumann F,Regli L,Levivier M,Hildebrandt G,Landolt H,Mariani L,Guzman R,Beck J,Raabe A,Keller E,Bijlenga P,Schaller K, Incidence and Outcome of Aneurysmal Subarachnoid Hemorrhage: The Swiss Study on Subarachnoid Hemorrhage (Swiss SOS). Stroke. 2021 Jan; [PubMed PMID: 33272133]
Al-Dhahir MA, Hall WA, Das JM, Sharma S. Neurogenic Pulmonary Edema. StatPearls. 2025 Jan:(): [PubMed PMID: 30422579]
Pratt AK, Chang JJ, Sederstrom NO. A Fate Worse Than Death: Prognostication of Devastating Brain Injury. Critical care medicine. 2019 Apr:47(4):591-598. doi: 10.1097/CCM.0000000000003647. Epub [PubMed PMID: 30855326]
Zheng K, Zhong M, Zhao B, Chen SY, Tan XX, Li ZQ, Xiong Y, Duan CZ. Poor-Grade Aneurysmal Subarachnoid Hemorrhage: Risk Factors Affecting Clinical Outcomes in Intracranial Aneurysm Patients in a Multi-Center Study. Frontiers in neurology. 2019:10():123. doi: 10.3389/fneur.2019.00123. Epub 2019 Feb 27 [PubMed PMID: 30873104]
Level 2 (mid-level) evidence