Introduction
Tuberculosis (TB) is a chronic granulomatous infection caused by species of mycobacteria, most commonly Mycobacterium tuberculosis (Mtb). TB has a worldwide distribution that is heavily weighted toward developing countries and is encountered infrequently in developed parts of the world. Mycobacteria are acid-fast, aerobic bacilli capable of affecting any organ, though the lungs are most commonly involved. Cutaneous tuberculosis (CTB) is a rare form of extrapulmonary TB, accounting for 1.5% to 3% of cases.[1][2][3][4] Mtb is responsible for a majority of CTB cases, Mycobacterium bovis, and bacillus Calmette-Guerin (BCG) are rare causes of the disease.TB is an ancient infectious disease dating back millennia. The first report of CTB is attributed to Rene Laennec, who, in 1826, described a lesion on his hand caused by direct inoculation resulting from the dissections he performed.[3] The causative organism was not identified until 1882, when Robert Koch discovered Mtb.[5] This activity will present clinical categories, epidemiology, pathophysiology, and the approach to diagnosis and treatment of CTB.
Classification
CTB is polymorphous. Lesion characteristics can appear as nodules, ulcers, infiltrated plaques, abscesses, verrucous papules and nodules, and a combination of the above. The classification of CTB is based on the route and propagation of infection, as well as the host's immune status. Depending on Mtb strain pathogenicity, previous exposure, and host immunity, CTB lesions can be multibacillary or paucibacillary and are categorized as true cutaneous TB or tuberculid. Within each of these categories, varying characteristic forms have been identified, including:
- True cutaneous TB
- Exogenous cutaneous tuberculosis (inoculation TB)
- Tuberculous chancre [No prior TB exposure]
- Tuberculosis verrucosa cutis [Previous TB immunity]
- Lupus vulgaris [Previous TB immunity]
- Post-BCG vaccination
- Subcutaneous abscess
- Regional lymphadenopathy
- Ulceration
- Keloid
- Lupus vulgaris
- Scrofuloderma
- Endogenous cutaneous tuberculosis (originating from a primary site of TB)
- Contiguity or autoinoculation [Low TB immunity]
- Scrofuloderma: arising from contiguous focus (eg, lymph node, bone, joint, epididymis)
- Tuberculous orificialis: arising from autoinoculation of mucocutaneous tissues (eg, oral, nasal, anogenital) from a primary TB focus
- Lupus vulgaris
- Hematogenous dissemination (low TB immunity)
- Lupus vulgaris
- Tuberculous gumma (ie, abscess)
- Acute miliary TB
- Tuberculid (hypersensitivity id like reaction to Mtb antigens)
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
CTB is caused by infection with the Mtb complex. Rarely, CTB can be caused by the attenuated strain of Mycobacterium bovis and the BCG vaccine.[2] See StatPearls companion resource, “Tuberculosis Overview,” for more information on the microbiology and etiology of tuberculosis.
Epidemiology
TB remains a global concern, infecting approximately 10 million people annually. Worldwide, TB is the leading cause of death from a single infectious disease, according to the World Health Organization (WHO).[WHO/tuberculosis] Most cases are concentrated in endemic areas, with India, China, Indonesia, Philippines, Pakistan, Nigeria, Bangladesh, and the Democratic Republic of the Congo accounting for more than two-thirds of global cases.[3] Consequently, endemic areas have higher rates of CTB, which represents about 1% to 3% of extrapulmonary tuberculosis. The incidence of disease is notably higher (approximately 6%) in parts of the world where infection with HIV is prevalent.[3]
Pathophysiology
Cutaneous forms of TB can develop from direct inoculation of the skin, contiguous spread from infected lymph nodes and organs to the skin, or hematogenous dissemination to the skin. CTB can also develop in the form of hypersensitivity reactions to Mtb antigens. As noted earlier, the clinical presentation of CTB is a function of the route of infection in conjunction with Mtb strain pathogenicity, prior exposure, and immune status of the host.[3][2][1][6] See StatPearls companion resource, “Tuberculosis Overview,” for more information on pulmonary and extrapulmonary TB pathophysiology.
Direct inoculation can result in tuberculous chancre in those without prior exposure and in TB verrucosa cutis or lupus vulgaris in those with some degree of TB immunity. Hematogenous dissemination can cause acute miliary CTB or TB gumma in the immune-compromised host and lupus vulgaris in those with some degree of TB immunity. Contiguous spread from lymph nodes, bones, and other organs can cause scrofuloderma or lupus vulgaris. Autoinoculation of mucosal tissues resulting in TB orificialis can occur in immune-compromised hosts with TB involving the gastrointestinal, respiratory, and genitourinary tracts. Tuberculids are considered type IV hypersensitivity reactions to Mtb antigens and infer that there is an underlying focus of active pulmonary or extrapulmonary TB.[7] The precise immunopathogenesis underlying CTB clinical presentations is complex and not fully elucidated.
Histopathology
The classic histopathological finding of CTB is the presence of tuberculoid granuloma. However, early lesions may present as a suppurative reaction characterized by a dense dermal infiltrate of neutrophils, lymphocytes, and plasma cells. Over time, a homogeneous eosinophilic necrotic center develops, with multinucleated giant cells palisading the caseation. Stains, eg, Ziehl-Neelsen, Fite-Faraco, Kinyoun, and Auramine-rhodamine, aid in determining the presence of acid-fast bacilli. The histopathological findings differ depending on the specific form of CTB. However, characteristic histology may be absent in up to 30% of cases.[6] The following findings may be demonstrated with these CTB manifestations:
- Tuberculous chancre: At the inoculation site the early stages demonstrate a suppurative infiltrate of neutrophils. Dermal necrosis may be present in the reticular dermis. Granulomas may develop in later stages. AFB stains are usually positive.
- TB verrucosa cutis: Pseudoepitheliomatous hyperplasia with hyperkeratosis is seen with microabscesses composed of neutrophils in the papillary dermis. Granulomas within the mid-dermis are often present. AFB stains are usually negative.
- Lupus vulgaris: Granulomas, whether tuberculoid or confluent, with central caseous necrosis, present in a quarter of cases. Granulomas can be surrounded by lymphocytes and plasma cells. Changes to the epidermis vary from acanthosis to hyperkeratosis. AFB stains are usually negative.
- Scrofuloderma: Tuberculoid granulomas have been a feature in all cases. Necrosis, giant cells, and neutrophilic abscesses are commonly present. AFB stains are usually positive.
- Orificial TB: The epidermal changes vary from ulceration to acanthosis. Caseating granulomas are commonly present. AFB stains are usually positive.
- Acute miliary TB: Similar to lupus vulgaris, the epidermal changes in acute miliary TB vary from hyperkeratosis to acanthosis or papillomatosis. Neutrophilic abscesses can be found in the dermis, where chronic inflammatory cells consist of lymphohistiocytic and plasma cell infiltrates. Necrosis is a common feature. AFB stains are usually positive.
- Tuberculous gumma: Granuloma may or may not form; however, diffuse histiocytic infiltrate is present. Casseation typically occurs in the reticular dermis. AFB stains are usually positive.
- Lichen scrofulosorum: The papillary dermis contains perifollicular granulomas. Caseation is absent. AFB stains are negative.
- Papulonecrotic tuberculid: Leukocytoclastic vasculitis and vascular occlusion are present in association with necrosis within the papillary dermis. Granulomas are rare. AFB stains are negative.
- Erythema induratum of Bazin: Lobular panniculitis, lymphocytic vasculitis, and fat necrosis in the presence or absence of epithelioid granuloma. AFB stains are negative.
History and Physical
The diagnosis of CTB requires vigilance and a high index of suspicion since its clinical presentation can mimic many inflammatory and neoplastic diseases. In areas of the world where TB prevalence is low, CTB is exceedingly rare and easily overlooked. A thorough history should include TB and HIV risk factors, country of origin, family history and known TB exposure, history of TB, BCG vaccination, occupational exposure, and localized trauma.
Since CTB can coexist with pulmonary and other extrapulmonary forms of TB, both history and physical examination should explore these possible manifestations. Systemic symptoms, eg, fever, malaise, anorexia, weight loss, and night sweats, occur in approximately 30% of cases.[1] Lymphadenopathy due to disseminated TB is common and should be explored during the physical examination. In addition to lymph nodes, TB-infected bones, joints, and epididymis may underlie lesions of scrofuloderma.
Tuberculous chancre
Tuberculous chancre (also known as primary inoculation tuberculosis) accounts for up to 1% of CTB. It typically presents as a red to brown papule that develops 2 to 4 weeks after mycobacteria enter the injury site. Over time, the lesion ulcerates, forming undermined borders. Chancres are generally painless. (see Image. Tuberculous Chancre).
Tuberculous verrucosa cutis
TB verrucosa cutis accounts for 3% to 19% of CTB cases. As the name suggests, it presents as a verrucous plaque. These lesions are usually found on the lower legs and feet, often due to kneeling on contaminated surfaces or walking barefoot. TB verrucosa cutis is typically diagnosed years after the initial injury because the lesion grows slowly and remains asymptomatic. (see Image. Tuberculosis Verrucosa Cutis).
Lupus vulgaris
Lupus vulgaris is the most common form of CTB, accounting for about 63% of cases. It can result from endogenous as well as exogenous sources of infection. In the latter case, inoculation via localized trauma, eg, ear piercing or placement of a tattoo by contaminated instruments, can result in lupus vulgaris lesions. Like TB verrucosa cutis, lupus vulgaris is slow-growing and asymptomatic, which leads to delayed diagnosis. The typical presentation is a red to brown plaque, with one border showing a scaly crust and the other showing scarring. The center of the lesions is often atrophic. Multiple plaques may arise and are typically found on the head, neck, arms, or legs. They can appear in a sporotrichoid pattern, where lesions spread along the lymphatic channels in a linear configuration. (see Image. Lupus Vulgaris Pretreatment and Posttreatment).
Scrofuloderma
Scrofuloderma is most common in endemic areas of developing countries such as Brazil and India. It most commonly presents in children as asymptomatic, indurated plaques that later ulcerate and drain purulent or caseous material. The ulcers often have violaceous borders. Scrofuloderma can present as a solitary lesion or multiple lesions, typically overlying cervical lymph nodes. It may also appear in other areas of infected lymph nodes and overlying infected bones, joints, and the scrotum. (see Image. Scrofuloderma Involving Bilateral Cervical Lymph Nodes).
Orificial tuberculosis
Orificial TB is a rare form of CTB that presents as a painful ulcer that does not heal. Due to self-inoculation in those with pulmonary TB or gastrointestinal involvement, this form is more commonly found in the oral cavity of immunosuppressed individuals. It can also occur in the nares, vulva, and peri-anal mucosa (see Image. Orificial Tuberculosis).
Miliary tuberculosis
Acute cutaneous miliary TB is a rare form but has the highest mortality rate. Individuals with this form of CTB often appear ill and present with multiple red papules and pustules that vary in size. Some papules can be umbilicated, and others may have necrotic centers. These lesions are commonly found on the trunk and extremities. There is an association with HIV/AIDS and other causes of immune suppression. (see Image. Miliary Cutaneous Tuberculosis).
Tuberculous gumma
Tuberculous gumma, also known as metastatic tuberculous abscess, is another rare form of CTB, typically seen in immunosuppressed individuals. It presents as multiple subcutaneous nodules that can ulcerate and develop sinus tracts. It is associated with a high mortality rate (see Image. Tuberculous Abscess).
BCG vaccination reactions and tuberculid lesions
BCG vaccination frequently causes a mild, localized, temporary skin reaction at the injection site. Abscess, chancre, fistula, and lupus vulgaris can rarely occur. Disseminated CTB has been rarely reported after BCG vaccination. The immunocompromised host is at the highest risk of this rare complication (see Image. Bacillus Calmette-Guérin Scar and Lymph Nodal Abscess and Progression).[4]
Tuberculid forms are due to a hypersensitivity reaction to Mtb antigens. Lichen scrofulosorum is seen most commonly in the pediatric population. It can present as perifollicular papules and coalescing lichenoid papules and plaques, often in a bilateral and symmetrical pattern on the trunk and lower extremities. It can also occur as a complication of BCG-associated lupus vulgaris.[4] Papulonecrotic tuberculid appears as painless, necrotic red-brown to violaceous papules and ulcers overlying extensor surfaces and develop most often on the trunk and extremities. Erythema induratum of Bazin presents as tender, erythematous subcutaneous nodules often appearing on the legs. The lesions can progress to ulcerate. It occurs predominantly in young women (see Images. Papulonecrotic Tuberculid and Erythema Induratum of Bazin in a 48-Year-Old Female).
Evaluation
When CTB is suspected, the following tests should be obtained:
- Skin biopsy with culture, histology, nucleic acid amplification test (NAAT), and AFB stain
- If scrofuloderma is suspected, a fine needle aspiration cytology along with stains, NAAT, and culture
- Interferon Gamma Release Assay (IGRA), particularly in those having received BCG vaccine or TB skin test if IGRA is not available
- A negative test does not preclude a diagnosis of CTB
- A positive test supports but does not confirm a diagnosis
- Complete blood count, metabolic panel, erythrocyte sedimentation rate
- HIV antibody test
- Focused screening tests for pulmonary and extrapulmonary TB, including chest x-ray, ultrasound, computed tomography (CT) scan, magnetic resonance imaging (MRI) scan
See StatPearls companion resource, “Tuberculosis Overview,” for more information on the diagnosis of TB.
Treatment / Management
Anti-tuberculosis therapy (ATT) for CTB is the same as for active pulmonary and extrapulmonary TB. A standard 4-drug regimen consisting of isoniazid, rifampicin, pyrazinamide, and ethambutol is administered for the first 2 months of intensive phase therapy. This is followed by a continuation phase of between 4 and 12 months with isoniazid and rifampin. The aforementioned assumes the presence of drug-sensitive TB. In the case of drug resistance, the ATT regimens require modifications in the agents and the duration of therapy.[1][6][4][8] See StatPearls companion resource, “Tuberculosis Overview,” for more information on the treatment of drug-sensitive and resistant TB. When clinicians have a strong clinical suspicion of CTB, and definitive results of stains, cultures, NAAT, and histology are not available, initiating a course of ATT is reasonable.[1] Most cases of CTB will show evidence of a response within 4 to 6 weeks.
The outcome of treatment for CTB depends on several factors, including the individual’s immune status, overall health, the stage of the disease, the type of cutaneous lesions, treatment adherence, duration of therapy, and any adverse effects experienced during treatment. Regarding the latter, the initiation of ATT requires close monitoring of potential adverse effects and drug interactions. See StatPearls companion resource, “Tuberculosis Overview,” for more information on ATT adverse effects and drug interactions.
Differential Diagnosis
The differential diagnoses of CTB are extensive. A complete list is beyond the scope of this activity; however, several excellent reviews are available on this topic.[1][3][4] Bacterial, fungal, parasitic, and other mycobacterial infections, neoplasia, autoimmune diseases, and drug eruption are conditions that can have similar presentation to CTB. The differential diagnoses also include:
- Syphilitic chancre
- Secondary syphilis
- Bacterial abscess
- Sporotrichosis
- Blastomycosis
- Nocardiosis
- Leishmaniasis
- Actinomycosis
- Sarcoid
- Psoriasis
- Discoid lupus
- Hidradenitis
- Squamous cell carcinoma
- Drug eruption
Prognosis
Overall, the prognosis of CTB is generally better than in individuals with internal organ involvement or immunocompromised individuals. However, even with aggressive treatment, the outcome may be poor in immunocompromised patients or those harboring drug-resistant organisms. Among the different forms of CTB, mortality rates are higher in tuberculous gumma (approximately 66%) and miliary CTB, with mortality rates reaching up to 75%.[6] Additionally, scarring is a common complication of healed CTB lesions. If untreated, lupus vulgaris can eventually undergo malignant transformation to squamous carcinoma.[6]
Deterrence and Patient Education
TB is a common infectious disease in many parts of the world, notably those regions lacking robust public health infrastructure. In endemic areas, improving public awareness about TB, including its cutaneous manifestations, is crucial to ensuring timely medical consultation and intervention.
However, TB is uncommon in resource-rich regions of the world. CTB is a relatively uncommon form of extrapulmonary TB and may go undiagnosed for prolonged periods due to a lack of recognition on the part of patients and clinicians. The lack of TB education and awareness in both patients and clinicians results in suboptimal implementation of prevention, diagnosis, and treatment strategies.
Diagnostic tests may lack sensitivity and specificity. Furthermore, adhering to prolonged and complicated courses of ATT can be challenging. Therefore, given the prolonged and complex nature of treatment, patients should be informed about the importance of completing therapy to prevent drug resistance and relapse.
Enhancing Healthcare Team Outcomes
Enhancing patient-centered care for CTB requires an interprofessional approach involving physicians, advanced practitioners, nurses, pharmacists, microbiologists, pathologists, and public health professionals. Given CTB’s rarity and polymorphous presentation, physicians and advanced practitioners must develop strong diagnostic skills to recognize its varied manifestations, ensuring timely identification and treatment. Strategies such as continued medical education and interprofessional case discussions can help bridge knowledge gaps and reduce diagnostic delays. Nurses play a critical role in patient education, assisting individuals to understand the importance of adherence to ATT, recognizing adverse effects, and addressing concerns that may impact compliance.
Effective interprofessional communication and care coordination are essential for improving patient outcomes and safety. Pharmacists ensure appropriate medication management, monitoring for drug interactions and adverse effects, while microbiologists and pathologists contribute to accurate diagnosis through laboratory testing. Public health professionals play a crucial role in tracking and preventing TB transmission, reinforcing the importance of treatment adherence, and facilitating access to care. Close collaboration between all healthcare professionals ensures a seamless approach to treatment, minimizes delays and enhances patient engagement. By fostering a coordinated effort, healthcare teams can optimize CTB management, improve adherence to ATT, and reduce disease burden and transmission.
Media
(Click Image to Enlarge)
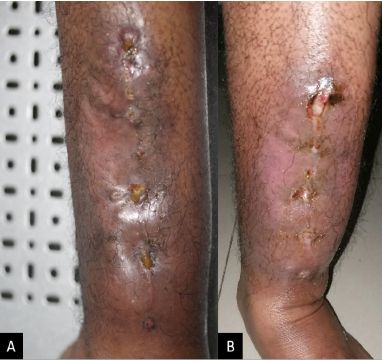
Tuberculous Chancre. Five months after a closed tibial fracture repair the patient developed a chronic nonhealing ulcer. The left tibia presents an ulcer characterized by a livid border and caseous secretion at the edge of the surgical wound (A). The surrounding area appears edematous and erythematous, indicating an inflammatory response (B).
Djawad K, Wahab S, Massi N. Coexistence of tuberculous chancre on a chronic nonhealing wound and bilateral submandibular scrofuloderma. Acta Dermatovenerol Alp Pannonica Adriat. 2021;30(2):79-81. doi: 10.15570/actaapa.2021.19.
(Click Image to Enlarge)

Tuberculosis Verrucosa Cutis. Inoculation of the skin of the knee in person from Nepal.
Contributed by R Tajhya, MD
(Click Image to Enlarge)

Lupus Vulgaris, Pre- and Posttreatment. This image on the left depicts a middle-aged woman with a diagnosis of Lupus Vulgaris (LV). The photograph highlights indurated and scarring plaque on her face before undergoing antituberculosis drug treatment. The image on the right shows significant improvement in the appearance of facial plaque, underlining the dramatic effects after 6 months of standard antituberculosis treatment.
Gallo JC, Claasens S, Visser WI, Jordaan HF, Schneider JW, Tod B. Cutaneous tuberculosis (lupus vulgaris-type). ID Cases. 2022;27:e01394. doi: 10.1016/j.idcr.2022.e01394.
(Click Image to Enlarge)

Scrofuloderma Involving Bilateral Cervical Lymph Nodes.
Djawad K, Wahab S, Massi N. Coexistence of tuberculous chancre on a chronic nonhealing wound and bilateral submandibular scrofuloderma. Acta Dermatovenerol Alp Pannonica Adriat. 2021;30(2):79-81.
doi: 10.15570/actaapa.2021.19.
(Click Image to Enlarge)

Orificial Tuberculosis. An ulcer is seen on the right lateral margin of the tongue.
Barragán YA, Murillo Cerda FJ, Vera MH, et al. Diagnosis of disseminated tuberculosis from a lesion in the oral cavity. IDCases. 2022;30:e01618. doi: 10.1016/j.idcr.2022.e01618.
(Click Image to Enlarge)

Miliary Cutaneous Tuberculosis. This image of the chest and upper limbs shows polymorphic dermatosis. Some plaques exhibit exulcerated areas and crusts with erythematous-violaceous borders. The middle image is a close-up view of the patient’s trunk exhibiting dermatosis and biopsy suture The right image is a close-up view of the patient’s right upper limb showing the patient's dermatosis. The patient is a 71-year-old immunocompromised host.
Arias Sepúlveda C, Hernandez Rivera KJ, Olaya Cordova M, et al. Unveiling a dermatological mystery: a rare case of miliary cutaneous tuberculosis in an adult patient. Cureus. 2024;16(9):e69854.
doi: 10.7759/cureus.69854.
(Click Image to Enlarge)
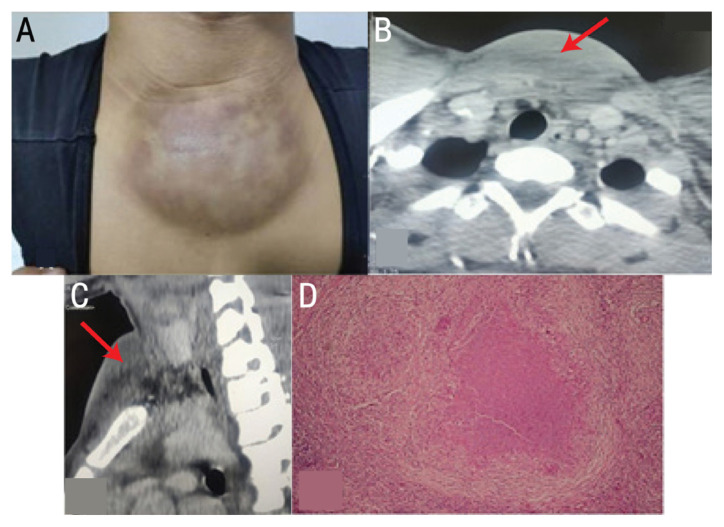
Tuberculous Abscess. This image of the neck of a 14-year-old boy shows a large fluctuant swelling in the suprasternal notch (A). A computed tomography scan of the neck and chest reveals a mass on suprasternal space (B, C). Hematoxylin and eosin stain at ×40 magnification shows a giganto-cellular granuloma with caseous necrosis (D). Acid-fast stains and mycobacterial cultures of biopsy tissue were negative. The nucleic acid amplification test was positive for Mtb. The child responded well to anti-tuberculosis therapy.
Bhairis M, El Hammoumi M, Kabiri M, Kabiri EH. Supra-sternal notch tuberculous abscess in child. Sultan Qaboos Univ Med J. 2023;23(4):562-563. doi: 10.18295/squmj.6.2023.042.
(Click Image to Enlarge)

Bacillus Calmette-Guérin Scar and Lymph Nodal Abscess and Progression. The image shows a BCG scar over the child’s right deltoid along with an accompanying lymph nodal abscess in the right axilla (A). The second image depicts resolved axillary swelling, indicating improvement after treatment (B).
Gautam U, Shrestha AL, Mishra A. Suppurative complications following BCG vaccine in 2 Nepalese children. Ann Med Surg (Lond). 2022;76:103484. doi: 10.1016/j.amsu.2022.103484.
(Click Image to Enlarge)

Papulonecrotic Tuberculid. The lesions appear over the ankle and tibia in this patient from Nepal.
Contributed by R Tajhya, MD
(Click Image to Enlarge)

Erythema Induratum of Bazin in a 48-Year-Old Female. She developed recurring painful lesions on bilateral calves 1.5 years before presenting for dermatology evaluation. She presented for dermatology evaluation 2 months after completing a 4-month regimen of rifampin for latent TB. A biopsy of a lesion showed lobular panniculitis with granulomatous inflammation and neutrophilic vasculitis.
Contributed by A Apple, MD
References
Kaul S, Kaur I, Mehta S, Singal A. Cutaneous tuberculosis. Part I: Pathogenesis, classification, and clinical features. Journal of the American Academy of Dermatology. 2023 Dec:89(6):1091-1103. doi: 10.1016/j.jaad.2021.12.063. Epub 2022 Feb 8 [PubMed PMID: 35149149]
Nguyen KH, Alcantara CA, Glassman I, May N, Mundra A, Mukundan A, Urness B, Yoon S, Sakaki R, Dayal S, Chowdhury T, Harshavardhan S, Ramanathan V, Venketaraman V. Cutaneous Manifestations of Mycobacterium tuberculosis: A Literature Review. Pathogens (Basel, Switzerland). 2023 Jul 8:12(7):. doi: 10.3390/pathogens12070920. Epub 2023 Jul 8 [PubMed PMID: 37513768]
Brito AC, Oliveira CMM, Unger DA, Bittencourt MJS. Cutaneous tuberculosis: epidemiological, clinical, diagnostic and therapeutic update. Anais brasileiros de dermatologia. 2022 Mar-Apr:97(2):129-144. doi: 10.1016/j.abd.2021.07.004. Epub 2022 Jan 4 [PubMed PMID: 34996655]
Level 2 (mid-level) evidenceMaloney ME, Cohen B. Cutaneous tuberculosis in the pediatric population: A review. JAAD international. 2023 Sep:12():105-111. doi: 10.1016/j.jdin.2023.05.001. Epub 2023 May 17 [PubMed PMID: 37404246]
Mousavi-Sagharchi SMA, Ghorbani A, Meskini M, Siadat SD. Historical examination of tuberculosis; from ancient affliction to modern challenges. Journal of infection and public health. 2025 Mar:18(3):102649. doi: 10.1016/j.jiph.2024.102649. Epub 2025 Jan 3 [PubMed PMID: 39826381]
Kaul S, Jakhar D, Mehta S, Singal A. Cutaneous tuberculosis. Part II: Complications, diagnostic workup, histopathologic features, and treatment. Journal of the American Academy of Dermatology. 2023 Dec:89(6):1107-1119. doi: 10.1016/j.jaad.2021.12.064. Epub 2022 Feb 8 [PubMed PMID: 35149148]
Dhattarwal N, Ramesh V. Tuberculids: A Narrative Review. Indian dermatology online journal. 2023 May-Jun:14(3):320-329. doi: 10.4103/idoj.idoj_284_22. Epub 2022 Dec 14 [PubMed PMID: 37266079]
Level 3 (low-level) evidenceBhandari A, Mahajan R, Ramesh V. Drug-resistance and its impact on cutaneous tuberculosis. Indian dermatology online journal. 2022 Sep-Oct:13(5):570-577. doi: 10.4103/idoj.idoj_27_22. Epub 2022 Sep 5 [PubMed PMID: 36304661]