 Anatomy, Head and Neck: Inferior Oblique Muscle
Anatomy, Head and Neck: Inferior Oblique Muscle
Introduction
Extraocular muscles (EOMs) are crucial for ocular movement. The superior and inferior obliques and the 4 recti work together to move the eyes in various directions (see Image. Oculomotor Nerve Pathway). The inferior oblique is almost entirely muscular, unlike the superior oblique, which is both muscular and tendinous. The inferior oblique is primarily responsible for the eye's external rotation. The muscle's secondary and tertiary actions are elevation and abduction, respectively.[1]
Inferior oblique overaction is a common cause of vertical strabismus and can be seen in conditions like infantile esotropia. Inferior oblique dysfunction can affect ocular torsion, leading to diplopia. Surgery on the inferior oblique is a common procedure to correct strabismus. Understanding the inferior oblique's anatomy and function is essential for diagnosing and managing various ocular conditions, particularly those involving eye movement and alignment.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The inferior oblique is the shortest of all the eye muscles, measuring approximately 37 mm long. Unlike all other EOMs, the inferior oblique does not originate from the annulus of Zinn or the common tendinous ring. Instead, this EOM arises from the orbital floor lateral to the nasolacrimal groove.[2]
The slender muscle continues from its origin, running along the inferior surface of the eye, passing between the floor of the orbit and the inferior rectus to eventually insert on the eye's posterior inferolateral surface. The inferior oblique's width at the insertion point varies, averaging 9 mm. The inferior oblique has 2 surfaces: the superior ocular and the inferior orbital surfaces.
The muscle is defined by its anterior and posterior border at the orbital groove. The inferior oblique tendon inserts in the sclera under the lateral rectus. The anterior border is about 10 mm from the lateral rectus insertion point, while the posterior border is 1 to 2 mm in front of the macula. The muscle itself is not only shorter than other EOMs, but its tendon, which measures 1 to 2 mm, is also shorter than its counterparts.[3]
The inferior oblique is responsible for extorsion, elevation, and abduction. The superior and inferior obliques are the only EOMs capable of depressing and elevating the adducted eye, respectively, due to their unique anatomical paths.
Embryology
The inferior oblique and the superior, inferior, and medial recti are derived from the prechordal mesoderm. The inferior oblique's embryological origin is distinct from the other EOMs, which develop from the mesodermal cells in the prechordal plate and cranial mesoderm in conjunction with migrating neural crest cells. Specifically, the inferior oblique arises from the mesenchymal tissue at the anterior inferomedial part of the orbit near the maxila's orbital surface.[4]
Around 7 to 8 weeks of gestation, the inferior oblique begins to form from a dense mesenchymal condensation near the infraorbital nerve. Unlike the extraocular rectus muscles, which have a common origin at the annulus of Zinn, the inferior oblique originates from a different region and lacks cartilaginous tissue at its origin. By 12 to 15 weeks of gestation, the inferior oblique's muscular origin appears, attaching to dense fibrous tissue and eventually merging with the posterior part of the sclera.[5]
The embryological origin of the inferior oblique involves the coordinated action of multiple genes and signaling pathways that regulate the migration, proliferation, and differentiation of myogenic precursor cells from the cranial mesoderm.[6] The paired box gene 3 (Pax3) has been demonstrated to be important in the early development of the EOMs. Pax3 is crucial for the migration and proliferation of myogenic precursor cells from the cranial mesoderm.
In addition, homeobox genes such as Lhx2 and Pitx2 have been explored in the specification and patterning of the EOMs. These genes influence the inferior oblique, in particular, during the morphogenesis of the ocular region. The interaction between these genes and the downstream signaling pathways, including Wnt and bone morphogenetic protein (BMP) pathways, orchestrates the formation and proper positioning of the inferior oblique.[7]
Blood Supply and Lymphatics
The inferior oblique is perfused by a medial muscular branch of the ophthalmic artery and the infraorbital artery. The ophthalmic artery, a branch of the internal carotid artery, supplies most of the EOMs. The infraorbital artery, a branch of the maxillary artery, provides additional blood supply.[8] The inferior orbital vein drains the muscle.
Lymph from the inferior oblique follows the general lymphatic flow within the ocular region. Lymph from the orbit and periorbital structures, including the EOMs, initially flows toward the preauricular (parotid) and submandibular nodes before draining into the deep cervical lymph nodes.[9]
Nerves
The inferior division of the oculomotor nerve (cranial nerve III) runs inferolaterally along the inferior rectus to innervate the inferior oblique. The nerve is approximately 27 mm long, running from the orbital apex to the inferior oblique. The nerve to the inferior oblique is the longest branch of the inferior division of the oculomotor nerve. The nerve enters the muscle through its orbital surface. The nerve to the inferior oblique has been measured to be approximately 1.04 mm on the right and 1.07 mm on the left.
Interestingly, the nerve accompanies an artery, vein, and fibrous tissue component. The terminal 8 mm of the nerve is encased in this fibrous component. Hence, innervation of the inferior oblique occurs through a neurofibrovascular bundle, a unique feature of this EOM. This feature is of particular anatomical importance in anterior transposition surgeries. The neurofibrovascular bundle serves as the origin for the inferior oblique and provides an ancillary origin for its posterior fibers after transposition.[10]
The oculomotor nerve's inferior division also carries parasympathetic fibers to the ciliary ganglion near the optic nerve. These fibers innervate the sphincter pupillae and ciliary muscles.[11]
Muscles
EOMs are specialized skeletal muscles. EOMs possess both slow tonic- and saccadic-type muscle fibers. Unlike other muscles, EOMs have a large nerve-fiber-to-skeletal-muscle-fiber ratio of 1:3 to 1:5. In contrast, other skeletal muscles typically only have 1:50 to 1:125.[12]
Physiologic Variants
Though rare, anatomical variations of EOMs include the absence or duplication of muscles and innervation or insertion anomalies. These variations can cause extraocular movement dysfunction and may require surgical evaluation. Congenital aplasia or hypoplasia of the inferior oblique can result from disruptions in the normal developmental processes.[13]
The inferior oblique exhibits anatomical variations more frequently than other EOMs. These variations include the following:
- Multiple muscle bellies: The inferior oblique may present with 2 or more muscle bellies, as documented by different studies.[14][15][16]
- Muscular bridge: Another notable variation is the presence of a muscular bridge between the inferior oblique and inferior rectus.[17]
- Obliquus accessorius inferior: This accessory muscle originates from the orbital apex and inserts near the inferior rectus insertion. Although functionally similar to the inferior rectus, this muscle is distinct in its anatomical origin and insertion.
- Insertion variations: While the inferior oblique typically has a close relationship with the inferior rectus at its insertion, case reports document instances of the inferior oblique inserting near or adjacent to the lateral rectus. These unusual insertion sites can affect the muscle's mechanical action on the eye.
Surgical Considerations
The inferior oblique externally rotates, elevates, and abducts the eye. Any injury to this muscle may result in strabismus, a significant misalignment of the eyes. While patients may develop compensatory mechanisms for this movement disability, surgical intervention is often required for cosmetic and functional correction.
Inferior oblique overaction exists in 70% of patients with esotropia and 30% of patients with exotropia. This condition is characterized by disproportionate elevation of the eye during adduction. Inferior oblique overaction can be categorized into primary and secondary types. Primary inferior oblique overaction is congenital or of unclear etiology, often associated with bilateral overaction leading to infantile esotropia.[18] Secondary overaction typically occurs unilaterally and results from a defect in the superior oblique, which normally controls abduction, internal rotation, and eye depression. Superior oblique paralysis leaves the inferior oblique unopposed, causing excessive elevation.
Surgical correction methods for inferior oblique overaction include disinsertion, extirpation and denervation, recession, myectomy, and anterior transposition of the muscle. The anterior transposition technique is particularly effective for patients with inferior oblique overaction with dissociated vertical deviation.[19][20] This procedure converts the inferior oblique into a depressor, significantly reducing its normal action and limiting upward gaze to 30° to 35°.[21]
A myectomy is performed in patients with vertical hypertropia without dissociated vertical deviation. This procedure is both prophylactic and cosmetic, as patients with inferior oblique overaction have an increased risk of developing retinal holes and tears due to the muscle's traction on the thin sclera. The inferior oblique is often transected during enucleation to provide traction to the globe (see Image. Eye Enucleation and the Inferior Oblique).
Clinical Significance
Inferior oblique dysfunction is often discovered by parents and pediatricians during infancy, allowing an early referral to an ophthalmologist. In the early stages, the condition is treated by patching the dominant eye, which forces the abnormal eye to compensate and strengthen. Surgical intervention is recommended if patching fails.[22]
Other Issues
The inferior oblique is susceptible to injury during lower blepharoplasty resection. Patients with postsurgical inferior oblique injury typically present with symptoms ranging from transient diplopia to permanent strabismus. Diplopia resulting from an inferior oblique injury usually manifests with a distorted visual image with an upward lateral gaze. Patients often unknowingly compensate by tilting their heads or lifting their chins.[23]
Media
(Click Image to Enlarge)
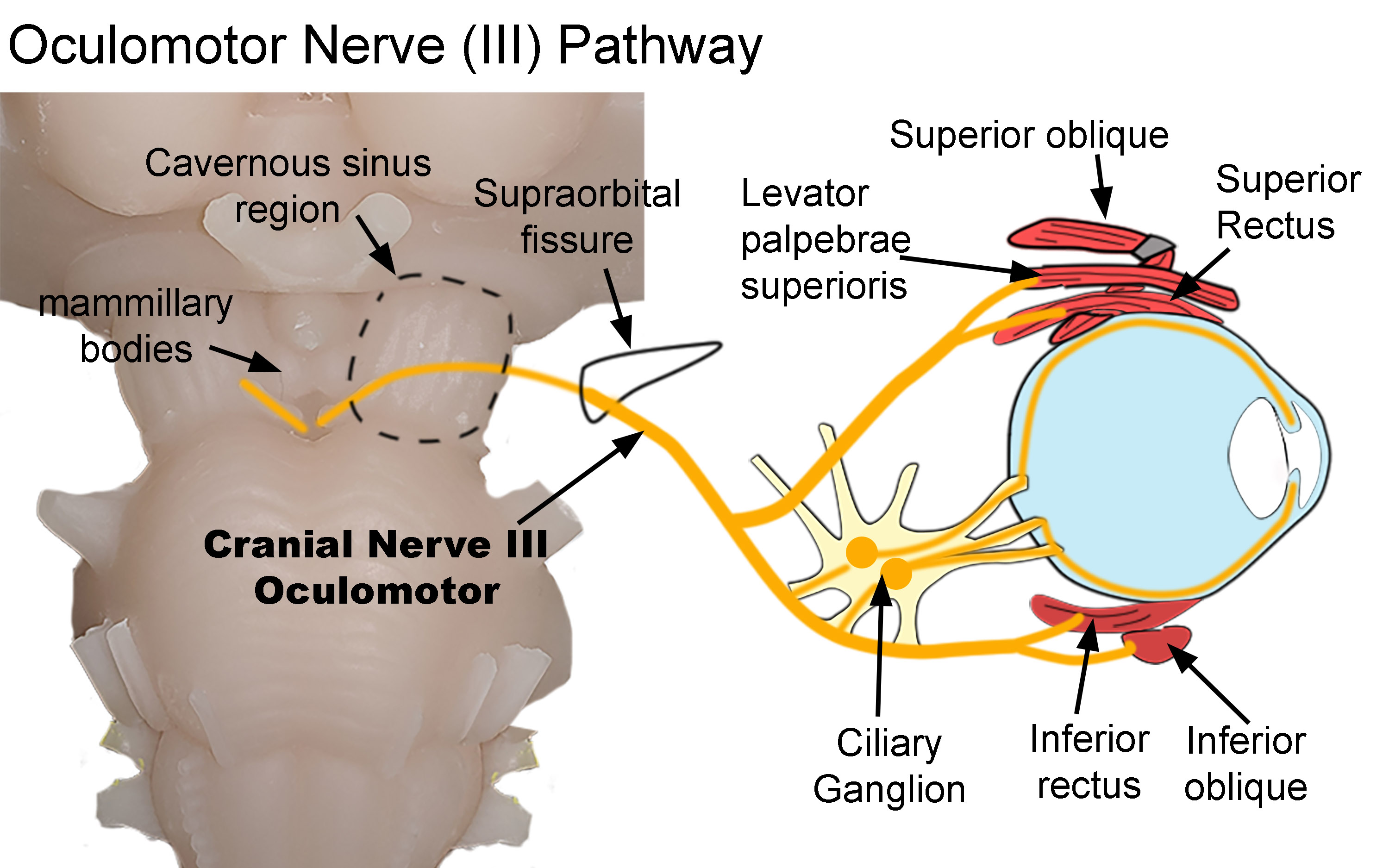
Oculomotor Nerve Pathway. The diagram shows the pathway of the oculomotor nerve as it exits the brainstem and terminates within the orbit. After exiting the brainstem, the nerve traverses both the cavernous sinus (dotted line) and supraorbital fissure (black line) before entering the orbit. Parasympathetic nerves synapse within the ciliary ganglion. Postganglionic nerves then innervate the sphincter papillae and ciliary muscles. Somatic nerves innervate the superior oblique, levator palpebrae superioris, superior and inferior recti, and inferior oblique.
Created by Diana Peterson, Ph.D. for use with StatPearls.
(Click Image to Enlarge)
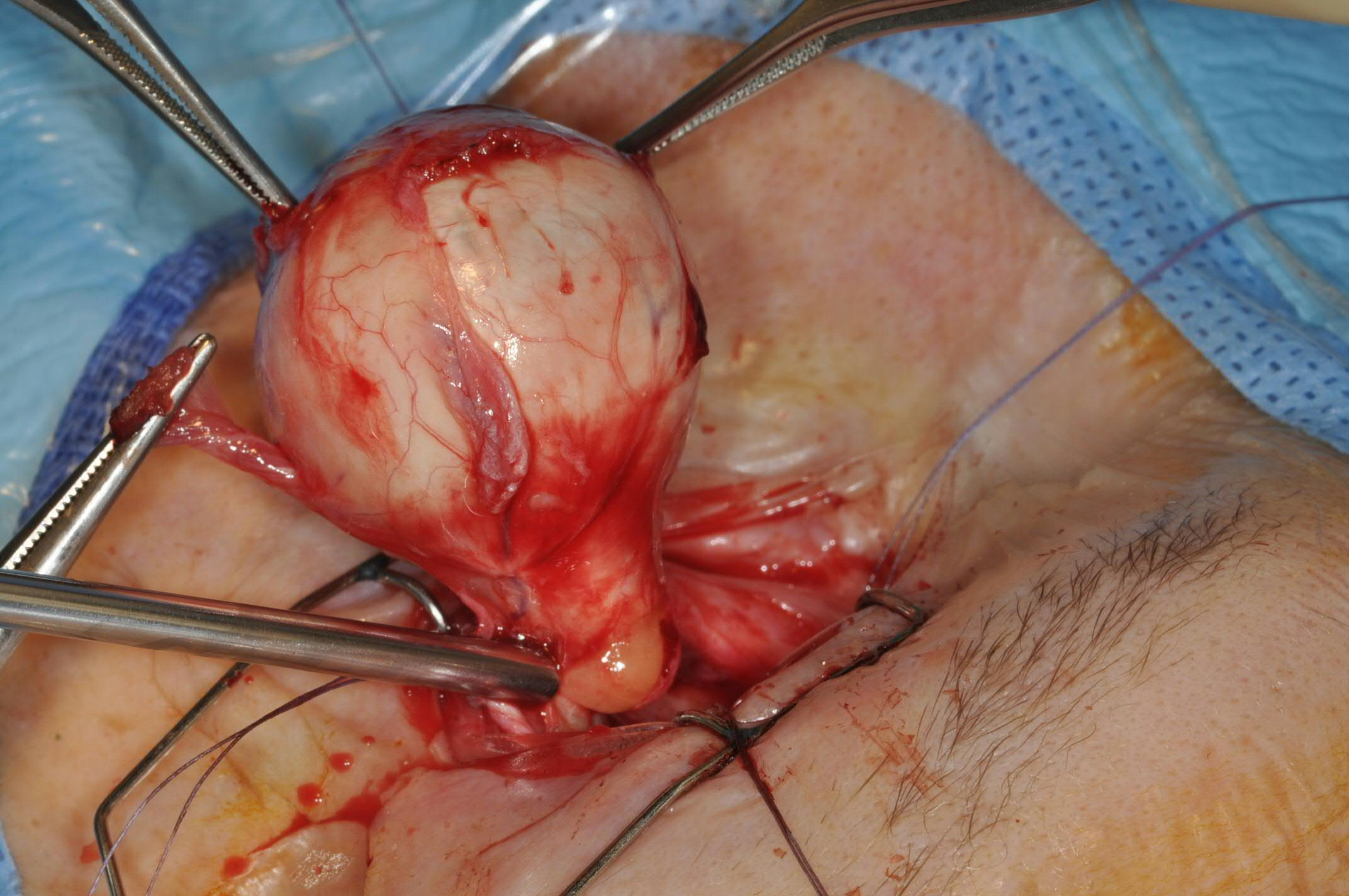
Eye Enucleation and the Inferior Oblique. The extraocular muscle may be used to provide traction to the globe, aiding the surgeon when cutting the optic nerve.
Contributed by Prof. Bhupendra C.K. Patel MD, FRCS
References
Stager D Jr, Dao LM, Felius J. Uses of the Inferior Oblique Muscle in Strabismus Surgery. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):292-7. doi: 10.4103/0974-9233.159723. Epub [PubMed PMID: 26180466]
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck, Eye Extraocular Muscles. StatPearls. 2024 Jan:(): [PubMed PMID: 30137849]
Kumar V, Murlimanju BV, Devika P, Nair N, Pai SR, Pulakunta T, Naveen NS. An anatomical study of the inferior oblique muscle with emphasis on its nerve entry. Chang Gung medical journal. 2011 May-Jun:34(3):293-7 [PubMed PMID: 21733359]
Haładaj R, Wysiadecki G, Polguj M, Topol M. Bilateral muscular slips between superior and inferior rectus muscles: case report with discussion on classification of accessory rectus muscles within the orbit. Surgical and radiologic anatomy : SRA. 2018 Jul:40(7):855-862. doi: 10.1007/s00276-018-1976-6. Epub 2018 Jan 24 [PubMed PMID: 29368252]
Level 3 (low-level) evidenceJin ZW, Umeki S, Takeuchi Y, Yamamoto M, Murakami G, Abe S, Rodríguez-Vázquez JF. Inferior oblique muscle of the eye: its foetal development with special reference to understanding of the frequent variants in adults. Folia morphologica. 2022:81(2):442-450. doi: 10.5603/FM.a2021.0043. Epub 2021 May 6 [PubMed PMID: 33954958]
Level 3 (low-level) evidenceBuckingham M. Gene regulatory networks and cell lineages that underlie the formation of skeletal muscle. Proceedings of the National Academy of Sciences of the United States of America. 2017 Jun 6:114(23):5830-5837. doi: 10.1073/pnas.1610605114. Epub [PubMed PMID: 28584083]
Hebert SL, Daniel ML, McLoon LK. The role of Pitx2 in maintaining the phenotype of myogenic precursor cells in the extraocular muscles. PloS one. 2013:8(3):e58405. doi: 10.1371/journal.pone.0058405. Epub 2013 Mar 7 [PubMed PMID: 23505501]
Gupta N, Motlagh M, Singh G. Anatomy, Head and Neck, Eye Arteries. StatPearls. 2024 Jan:(): [PubMed PMID: 30725748]
Mojallal A, Cotofana S. Anatomy of lower eyelid and eyelid-cheek junction. Annales de chirurgie plastique et esthetique. 2017 Oct:62(5):365-374. doi: 10.1016/j.anplas.2017.09.007. Epub 2017 Oct 14 [PubMed PMID: 29033216]
Stager DR. The neurofibrovascular bundle of the inferior oblique muscle as its ancillary origin. Transactions of the American Ophthalmological Society. 1996:94():1073-94 [PubMed PMID: 8981719]
Erdogmus S, Govsa F, Celik S. Innervation features of the extraocular muscles. The Journal of craniofacial surgery. 2007 Nov:18(6):1439-46 [PubMed PMID: 17993897]
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck: Eye Superior Rectus Muscle. StatPearls. 2024 Jan:(): [PubMed PMID: 30252323]
Shahraki K, Hakimeh C, Suh DW. Modified horizontal muscle transposition without tenotomy and splitting for a case of inferior rectus and inferior oblique muscles aplasia with hemifacial microsomia. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2023 Dec:27(6):354-357. doi: 10.1016/j.jaapos.2023.07.015. Epub 2023 Sep 22 [PubMed PMID: 37741493]
Level 3 (low-level) evidenceDeangelis DD, Kraft SP. The double-bellied inferior oblique muscle: clinical correlates. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2001 Apr:5(2):76-81 [PubMed PMID: 11304813]
Yalçin B, Ozan H. Insertional pattern of the inferior oblique muscle. American journal of ophthalmology. 2005 Mar:139(3):504-8 [PubMed PMID: 15767061]
De Angelis D, Makar I, Kraft SP. Anatomic variations of the inferior oblique muscle: a potential cause of failed inferior oblique weakening surgery. American journal of ophthalmology. 1999 Oct:128(4):485-8 [PubMed PMID: 10577590]
Yalçin B, Kocabiyik N, Ozan H, Kutoglu T. Muscular bridge between the inferior oblique and inferior rectus muscles. American journal of ophthalmology. 2004 Jan:137(1):121-4 [PubMed PMID: 14700654]
Sanjari MS, Shahraki K, Nekoozadeh S, Tabatabaee SM, Shahraki K, Aghdam KA. Surgical treatments in inferior oblique muscle overaction. Journal of ophthalmic & vision research. 2014 Jul-Sep:9(3):291-5. doi: 10.4103/2008-322X.143355. Epub [PubMed PMID: 25667727]
Stager DR, Weakley DR Jr, Stager D. Anterior transposition of the inferior oblique. Anatomic assessment of the neurovascular bundle. Archives of ophthalmology (Chicago, Ill. : 1960). 1992 Mar:110(3):360-2 [PubMed PMID: 1543454]
Rajavi Z, Feizi M, Behradfar N, Yaseri M, Sayanjali S, Motevaseli T, Sabbaghi H, Faghihi M. Inferior Oblique Overaction: Anterior Transposition Versus Myectomy. Journal of pediatric ophthalmology and strabismus. 2017 Jul 1:54(4):232-237. doi: 10.3928/01913913-20170309-01. Epub 2017 May 17 [PubMed PMID: 28510770]
Stager DR. Costenbader lecture. Anatomy and surgery of the inferior oblique muscle: recent findings. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2001 Aug:5(4):203-8 [PubMed PMID: 11507578]
Sokeer SH, Ali AL, Arafa ES, Awara AM, Shafik HM. Evaluation of graded recession of inferior oblique muscle for correction of different grades of V-pattern strabismus. BMC ophthalmology. 2023 Nov 16:23(1):462. doi: 10.1186/s12886-023-03210-x. Epub 2023 Nov 16 [PubMed PMID: 37974078]
Mowlavi A, Neumeister MW, Wilhelmi BJ. Lower blepharoplasty using bony anatomical landmarks to identify and avoid injury to the inferior oblique muscle. Plastic and reconstructive surgery. 2002 Oct:110(5):1318-22; discussion 1323-4 [PubMed PMID: 12360075]