Introduction
The striate arteries comprise small, penetrating vessels that originate from the anterior (ACA) and middle (MCA) cerebral arteries, delivering blood to deep cerebral structures, including the basal ganglia and internal capsule. The branching patterns and territories of these blood vessels demonstrate considerable anatomical variability across individuals. Despite their small caliber, these arteries play a critical role in sustaining motor function through perfusion of corticospinal and extrapyramidal fiber tracts (see Image. Striate Arteries and Deep Perforators).
Absence of significant collateral circulation renders this vascular territory highly vulnerable to lacunar infarction. Striate artery hypertrophy contributes to the pathogenesis of Moyamoya disease and warrants careful consideration during neurosurgical interventions involving the anterior circle of Willis. Injury to these vessels during aneurysm clipping or tumor resection can result in profound motor deficits due to infarction of the internal capsule. A thorough understanding of striate artery anatomy and function informs both clinical management of cerebrovascular disease and operative strategies aimed at preserving deep cerebral structures.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The striate arteries consist of a collection of small-caliber arteries branching from the anterior circle of Willis. These vessels supply the subcortical structures of the central nervous system.
The lenticulostriate arteries (LSAs) branch from the MCA, a vessel that originates from the internal carotid artery (ICA) and courses laterally along the inferior surface of the frontal lobe as the M1 segment, heading toward the lateral sulcus between the frontal and temporal lobes. Between 6 and 12 small-diameter LSAs arise from the M1 segment, supplying the internal capsule and basal ganglia. These branches range in diameter from 0.08 mm to 1.4 mm, with an average of 0.47 mm.[1][2]
The recurrent artery of Heubner (RAH), also known as the distal medial striate artery, is a specific striate branch of the ACA (see Image. Recurrent Artery of Heubner). After the ICA gives rise to the ACA, the A1 segment extends to its bifurcation into the A2 segment and the anterior communicating artery (ACoA). The RAH originates from either the distal portion of A1 or the proximal portion of A2.[3][4] The RAH follows a recurrent course in 60% of individuals, traveling anteriorly and inferiorly along the undersurface of the frontal lobe to the ICA bifurcation before entering the brain.[5] Vascular supply from the RAH reaches the septal nuclei, putamen, and anterior limb of the internal capsule. The RAH also serves as the primary, and often sole, arterial supply to the nucleus accumbens.[6] Average vessel diameter is 0.7 mm, with a length of approximately 24 mm.[7]
Striate arteries arising from both the ACA and MCA ascend through the anterior perforated substance of the basal forebrain. The anterior perforated substance is a region of grey matter bordered by the gyrus rectus, lateral olfactory striae, optic chiasm, and optic tract. Numerous small openings within this region are formed by the penetrating striate arteries.
Classification into lateral and medial striate arteries varies among sources and may lead to terminological confusion. One convention designates medial striate arteries, such as the RAH, as branches of the ACA, and lateral striate arteries as those arising from the M1 segment of the MCA. An alternative scheme defines medial and lateral striate arteries based on origin along the proximal versus distal M1 segment, respectively.[8]
Embryology
At the 4- to 5-mm stage, corresponding to approximately 28 to 30 days of gestation, the cranial division of the fetal ICA is referred to as the "primitive olfactory artery" (POA), reflecting its initial termination in the olfactory region of the developing brain.[9] As the POA extends toward the olfactory bulb, it gives rise to a small recurrent branch that later develops into the RAH. The POA subsequently gives rise to the ACA. By the 12- to 14-mm stage, the ACoA emerges from the distal ACA, completing the anterior component of the circle of Willis.
The MCAs begin to form between the 7- to 12-mm stage, at approximately 34 to 36 days, initially as multiple small vascular plexuses sprouting from the ICA. These plexuses coalesce into a single trunk at the 16- to 18-mm stage, near 39 to 41 days of development.[10] As the frontal and temporal lobes expand and the lateral fissure takes shape, cortical branches of the MCA form and penetrate the anterior perforated substance to supply deep cerebral structures.[11] The MCA achieves its definitive anatomical configuration by the 40-mm stage.[12]
Blood Supply and Lymphatics
Striate artery perfusion exhibits substantial interindividual variability. However, characteristic vascular territories can be identified. Lateral LSAs typically supply the caudate nucleus, putamen, globus pallidus, posterior limb and genu of the internal capsule, substantia innominata, lateral aspect of the anterior commissure, and the border zone of the corona radiata. Medial LSAs also perfuse the caudate nucleus, putamen, globus pallidus, and internal capsule. The RAH supplies the anteromedial caudate nucleus, putamen, globus pallidus, anterior limb of the internal capsule, septal nuclei, and nucleus accumbens.[13] In most cases, the RAH gives rise to the most medial and anterior perforating arteries, whereas LSAs arising from the MCA perfuse the middle and posterior components of the basal ganglia.[14]
Venous drainage from these deep cerebral structures occurs through the internal cerebral and basal veins. These vessels converge into the great vein of Galen, which subsequently drains into the straight dural sinus.[15]
Physiologic Variants
LSAs may occasionally arise from a large common trunk. Although this variant is usually of no clinical consequence, occlusion of the trunk may result in infarction of the entire dependent territory, producing a massive central hemispheric stroke. While LSAs typically originate from the M1 segment of the MCA, origins at the MCA bifurcation or along the M2 segment are also common. LSAs frequently arise from the accessory trunk in patients with accessory MCAs.
The origin of the RAH demonstrates marked interpatient variability. In 58% of cases, the RAH arises from the A2 segment within 5 mm of the ACoA bifurcation. An additional 30% originate from the A1 segment, and 12% diverge from the ACA-ACoA junction. A single RAH is most often present, though double, triple, or quadruple vessels have been observed. Unilateral or bilateral absence of the RAH has also been documented.[16]
Surgical Considerations
MCA aneurysms account for approximately 18% of all intracranial saccular aneurysms. Over 80% occur at terminal or false bifurcations, where the LSAs originate in 23% of patients. In these cases, the aneurysm may stretch, compress, or otherwise distort the striate arteries.[17] Iatrogenic injury to the RAH or LSAs can occur during endovascular surgery involving aneurysms of the ACA, ACoA, or MCA. Particular care is required to identify and preserve these vessels.[18][19][20][21][22] Intraoperative microscopic inspection is insufficient for assessing the patency of the perforators. Motor evoked potential monitoring is recommended to evaluate real-time perfusion.[23][24] Vascular injury may result in striatal infarctions, manifesting as transient or permanent brachiofacial hemiparesis, aphasia, or emotional dysregulation.
Aneurysms involving the LSAs or RAH are rare and typically present with subarachnoid or intracerebral hemorrhage.[25][26][27] Reported causes include hypertension, substance abuse, systemic lupus erythematosus, vascular malformations, and Moyamoya disease, although most cases are idiopathic.[28][29] Management strategies include coiling, clipping, embolization, radiosurgery, and surgical resection.[30] Preservation of the affected artery is often challenging due to its small caliber, and failure to do so may result in permanent neurologic sequelae.[31]
Neurosurgical evaluation is warranted in patients with Moyamoya disease. Moyamoya is a relatively rare cerebrovascular disorder characterized by luminal thrombosis and smooth muscle cell hyperplasia involving the intracranial portion of the ICA, as well as the proximal segments of the ACA and MCA. These changes lead to progressive stenosis and eventual occlusion.[32][33][34] Reduced cerebral perfusion triggers compensatory proliferation, dilatation, and collateralization of the striate arteries, along with choroidal and thalamoperforating vessels.[35][36] Abnormally increased flow through the small-caliber striate arteries may result in endothelial injury and formation of microaneurysms, increasing the risk for both ischemic and hemorrhagic complications.
Moyamoya follows a bimodal age distribution, with incidence peaks in childhood and midadulthood, and shows a higher prevalence in women and Asian populations.[37][38] Clinical manifestations include headache, chorea, seizures, transient ischemic attack, stroke, and intracranial hemorrhage. Although antiplatelet agents are commonly used, medical management alone fails to prevent disease progression. Consequently, neurosurgical intervention plays a central role in reducing long-term neurologic disability.
Surgical treatment primarily involves direct or indirect revascularization using the external carotid artery to augment flow to ischemic regions. Procedures include direct superficial temporal artery-to-MCA bypass, encephaloduroarteriosynangiosis, encephalomyosynangiosis, and the multiple burr holes technique.[39]
Clinical Significance
Striate arteries lack a significant collateral blood supply and are classified as end arteries, rendering them highly vulnerable to hypoxic injury. Ischemic strokes involving these vessels, known as lacunar infarcts, account for approximately 25% of all cerebral infarctions.[40] Lacunar infarcts are small ischemic lesions, typically measuring up to 15 or 20 mm, characterized by cavitary spaces, or lacunae, within the affected subcortical structures. By definition, lacunar strokes do not produce cortical signs such as aphasia, visual field deficits, visuospatial neglect, or gaze deviation. Clinical presentation may be silent or fall within 1 of 5 recognized lacunar stroke syndromes.
Pure motor stroke is the most common lacunar syndrome, comprising 1/3 to 1/2 of all presentations. Infarction typically involves the posterior limb of the internal capsule, corona radiata, or basilar pons. Resulting deficits include contralateral hemiparesis or hemiplegia of the face, arm, or leg. Ataxic hemiparesis is the 2nd most frequent lacunar syndrome. Infarction affects the regions implicated in pure motor stroke, with additional involvement of the lentiform and red nuclei. Symptoms include ipsilateral weakness and impaired coordination, most often affecting the lower extremity.
Dysarthria-clumsy hand syndrome results from infarction of the anterior limb or genu of the internal capsule, basilar pons, corona radiata, thalamus, basal ganglia, or cerebral peduncle. This presentation is characterized by dysarthria and hand clumsiness, particularly during fine motor tasks such as writing. Pure sensory stroke arises from infarction involving the ventral posterolateral nucleus of the thalamus, corona radiata, internal capsule, or midbrain. Clinical features include unilateral numbness and dysesthesias without motor involvement. Mixed sensorimotor stroke reflects the combined involvement of both sensory and motor pathways. Infarction typically affects the thalamus, posterior limb of the internal capsule, or lateral aspect of the pons. Manifestations may include contralateral hemiparesis or hemiplegia accompanied by sensory deficits.[41]
Multiple etiologies contribute to lacunar infarction. Intracranial atherosclerosis is believed to be the most common cause, often presenting as luminal or mural atheroma of the ACA or MCA that occludes the origin of a striate artery, junctional atheroma at the arterial origin, or microatheroma within the proximal segment of a perforator. These atheromatous lesions frequently result in stenosis or occlusion of the LSA or RAH. Atheroma-related occlusions typically involve arteries measuring 0.2 to 0.8 mm in diameter and produce symptomatic infarcts exceeding 5 mm.
Striate arteries are particularly susceptible to hypertension-induced injury, leading to segmental lipohyalinosis of the penetrating vessels. Chronic hypertension impairs cerebrovascular autoregulation and causes endothelial dysfunction, promoting extravasation of plasma components into the tunica media. This process triggers inflammation and fibrinoid necrosis, resulting in progressive stenosis of the striate arteries. Histologically, lipohyalinosis appears as homogeneous eosinophilic deposits that thicken the vessel wall. This pathology most commonly affects smaller arteries measuring 0.04 to 0.2 mm in diameter, producing asymptomatic infarcts typically 3 to 7 mm in size. Affected vessels are also structurally weakened and prone to rupture, leading to intracerebral hemorrhage.[42]
In patients without microvascular disease, lacunar infarcts may result from embolic occlusion. Carotid or cardiac emboli may enter the MCA and lodge at LSA branch points near the lateral sulcus.[43] The acute angulation between the ICA and MCA origin favors embolic flow into MCA territory, increasing the likelihood of striate artery involvement.
Media
(Click Image to Enlarge)
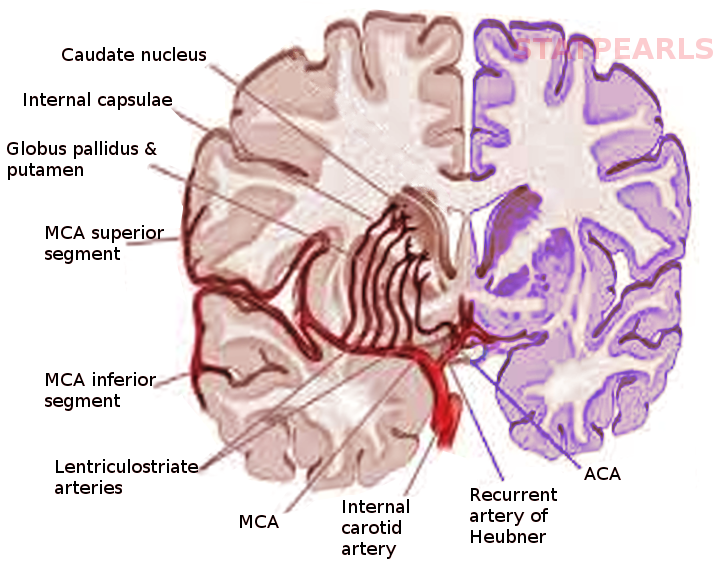
Striate Arteries and Deep Perforators. Coronal section showing the origin and distribution of the lenticulostriate arteries from the middle cerebral artery and the recurrent artery of Heubner from the anterior cerebral artery. These vessels supply the caudate nucleus, putamen, globus pallidus, and internal capsule.
Image courtesy S Bhimji MD
(Click Image to Enlarge)
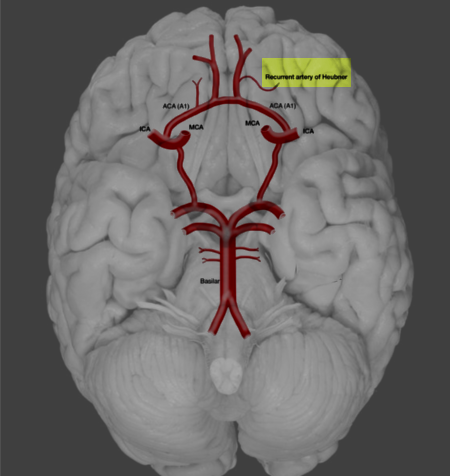
Recurrent Artery of Heubner. This illustration shows the location and course of the recurrent artery of Heubner.
Image courtesy O. Chaigasame
References
Marinkovic S, Gibo H, Milisavljevic M, Cetkovic M. Anatomic and clinical correlations of the lenticulostriate arteries. Clinical anatomy (New York, N.Y.). 2001 May:14(3):190-5 [PubMed PMID: 11301466]
Djulejić V, Marinković S, Milić V, Georgievski B, Rašić M, Aksić M, Puškaš L. Common features of the cerebral perforating arteries and their clinical significance. Acta neurochirurgica. 2015 May:157(5):743-54; discussion 754. doi: 10.1007/s00701-015-2378-8. Epub 2015 Mar 14 [PubMed PMID: 25772345]
Zunon-Kipré Y, Peltier J, Haïdara A, Havet E, Kakou M, Le Gars D. Microsurgical anatomy of distal medial striate artery (recurrent artery of Heubner). Surgical and radiologic anatomy : SRA. 2012 Jan:34(1):15-20. doi: 10.1007/s00276-011-0888-5. Epub 2011 Nov 25 [PubMed PMID: 22116404]
Kang HS, Han MH, Kwon BJ, Kwon OK, Kim SH, Chang KH. Evaluation of the lenticulostriate arteries with rotational angiography and 3D reconstruction. AJNR. American journal of neuroradiology. 2005 Feb:26(2):306-12 [PubMed PMID: 15709128]
Level 2 (mid-level) evidenceMansfield K, Rahme R. Dissecting Aneurysm of the Recurrent Artery of Heubner in a Patient With Osteogenesis Imperfecta. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 2015 Nov:42(6):461-5. doi: 10.1017/cjn.2015.295. Epub [PubMed PMID: 26551090]
Mavridis I, Anagnostopoulou S. Comment on the brain areas whose blood supply is provided by the recurrent artery of Heubner. Surgical and radiologic anatomy : SRA. 2010 Jan:32(1):91. doi: 10.1007/s00276-009-0540-9. Epub 2009 Aug 14 [PubMed PMID: 19688287]
Level 3 (low-level) evidenceLoukas M, Louis RG Jr, Childs RS. Anatomical examination of the recurrent artery of Heubner. Clinical anatomy (New York, N.Y.). 2006 Jan:19(1):25-31 [PubMed PMID: 16287124]
Reyes Soto G, Pérez Cruz JC, Nikolenko V, Rosario Rosario A, Mpoyi Chérubin T, Güngör A, Castillo Rangel C, Encarnacion Ramirez MJ. Microsurgical insights: A comprehensive anatomical study of Heubner's recurrent artery. Surgical neurology international. 2025:16():158. doi: 10.25259/SNI_81_2025. Epub 2025 May 2 [PubMed PMID: 40469350]
Bertulli L, Robert T. Embryological development of the human cranio-facial arterial system: a pictorial review. Surgical and radiologic anatomy : SRA. 2021 Jun:43(6):961-973. doi: 10.1007/s00276-021-02684-y. Epub 2021 Jan 25 [PubMed PMID: 33492439]
Kathuria S, Gregg L, Chen J, Gandhi D. Normal cerebral arterial development and variations. Seminars in ultrasound, CT, and MR. 2011 Jun:32(3):242-51. doi: 10.1053/j.sult.2011.02.002. Epub [PubMed PMID: 21596279]
Okahara M, Kiyosue H, Mori H, Tanoue S, Sainou M, Nagatomi H. Anatomic variations of the cerebral arteries and their embryology: a pictorial review. European radiology. 2002 Oct:12(10):2548-61 [PubMed PMID: 12271398]
Uchiyama N. Anomalies of the Middle Cerebral Artery. Neurologia medico-chirurgica. 2017 Jun 15:57(6):261-266. doi: 10.2176/nmc.ra.2017-0043. Epub 2017 Apr 27 [PubMed PMID: 28450666]
Djulejić V, Marinković S, Georgievski B, Stijak L, Aksić M, Puškaš L, Milić I. Clinical significance of blood supply to the internal capsule and basal ganglia. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2016 Mar:25():19-26. doi: 10.1016/j.jocn.2015.04.034. Epub 2015 Nov 16 [PubMed PMID: 26596401]
Feekes JA, Cassell MD. The vascular supply of the functional compartments of the human striatum. Brain : a journal of neurology. 2006 Aug:129(Pt 8):2189-201 [PubMed PMID: 16815876]
Uddin MA, Haq TU, Rafique MZ. Cerebral venous system anatomy. JPMA. The Journal of the Pakistan Medical Association. 2006 Nov:56(11):516-9 [PubMed PMID: 17183980]
El Falougy H, Selmeciova P, Kubikova E, Haviarová Z. The variable origin of the recurrent artery of Heubner: an anatomical and morphometric study. BioMed research international. 2013:2013():873434. doi: 10.1155/2013/873434. Epub 2013 Jul 9 [PubMed PMID: 23936853]
Park JC, Shim JH, Lee DH, Ahn JS, Lee DG, Yang K, Park W, Koo HW, Jiang YY, Kwon do H, Kwun BD. Three-Dimensional Angiographic Evaluation of Middle Cerebral Artery Trunk Aneurysms: Demonstration of the Close Relationship Between the Early Frontal Cortical Branches and Lateral Lenticulostriate Arteries. World neurosurgery. 2016 Jul:91():383-9. doi: 10.1016/j.wneu.2016.04.065. Epub 2016 Apr 27 [PubMed PMID: 27132178]
Mugikura S, Kikuchi H, Fujimura M, Mori E, Takahashi S, Takase K. Subcallosal and Heubner artery infarcts following surgical repair of an anterior communicating artery aneurysm: a causal relationship with postoperative amnesia and long-term outcome. Japanese journal of radiology. 2018 Feb:36(2):81-89. doi: 10.1007/s11604-017-0703-2. Epub 2017 Nov 23 [PubMed PMID: 29170982]
Hashimoto Y, Tsushima S, Komeichi T, Niwa J. [Contralateral infarction in the territory of the recurrent artery of Heubner after anterior communicating artery aneurysm surgery]. No shinkei geka. Neurological surgery. 2008 Sep:36(9):813-7 [PubMed PMID: 18800637]
Level 3 (low-level) evidenceMatano F, Murai Y, Tateyama K, Mizunari T, Umeoka K, Koketsu K, Kobayashi S, Teramoto A. Perioperative complications of superficial temporal artery to middle cerebral artery bypass for the treatment of complex middle cerebral artery aneurysms. Clinical neurology and neurosurgery. 2013 Jun:115(6):718-24. doi: 10.1016/j.clineuro.2012.08.007. Epub 2012 Aug 22 [PubMed PMID: 22921036]
Level 3 (low-level) evidenceNishioka H, Haraoka J, Miki T, Akimoto J, Yamanaka S, Hasegawa K, Matsumura H. [Surgical treatment of proximal middle cerebral artery (M1) aneurysms at the origin of the lenticulostriate artery]. No shinkei geka. Neurological surgery. 2003 Jan:31(1):27-33 [PubMed PMID: 12533902]
Level 3 (low-level) evidenceChoque-Velasquez J, Hernesniemi J. Microsurgical clipping of a large ruptured anterior communicating artery aneurysm. Surgical neurology international. 2018:9():233. doi: 10.4103/sni.sni_345_18. Epub 2018 Nov 28 [PubMed PMID: 30595954]
Sasaki T, Kodama N, Matsumoto M, Suzuki K, Konno Y, Sakuma J, Endo Y, Oinuma M. Blood flow disturbance in perforating arteries attributable to aneurysm surgery. Journal of neurosurgery. 2007 Jul:107(1):60-7 [PubMed PMID: 17639875]
Horiuchi K, Suzuki K, Sasaki T, Matsumoto M, Sakuma J, Konno Y, Oinuma M, Itakura T, Kodama N. Intraoperative monitoring of blood flow insufficiency during surgery of middle cerebral artery aneurysms. Journal of neurosurgery. 2005 Aug:103(2):275-83 [PubMed PMID: 16175857]
Vellore Y, Madan A, Hwang PY. Recurrent artery of Heubner aneurysm. Asian journal of neurosurgery. 2014 Oct-Dec:9(4):244. doi: 10.4103/1793-5482.146658. Epub [PubMed PMID: 25685237]
Level 3 (low-level) evidenceVargas J, Walsh K, Turner R, Chaudry I, Turk A, Spiotta A. Lenticulostriate aneurysms: a case series and review of the literature. Journal of neurointerventional surgery. 2015 Mar:7(3):194-201. doi: 10.1136/neurintsurg-2013-010969. Epub 2014 Feb 26 [PubMed PMID: 24574545]
Level 3 (low-level) evidenceChoo YS, Kim YB, Shin YS, Joo JY. Deep Intracerebral Hemorrhage Caused by Rupture of Distal Lenticulostriate Artery Aneurysm : A Report of Two Cases and a Literature Review. Journal of Korean Neurosurgical Society. 2015 Nov:58(5):471-5. doi: 10.3340/jkns.2015.58.5.471. Epub 2015 Nov 30 [PubMed PMID: 26713149]
Level 3 (low-level) evidenceAgarwalla PK, Walcott BP, Dunn IF, Thiex R, Frerichs K, Narang S, Friedlander RM. Fusiform aneurysms of the lenticulostriate artery. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2014 Mar:21(3):373-7. doi: 10.1016/j.jocn.2013.07.009. Epub 2013 Oct 21 [PubMed PMID: 24156904]
Lama S, Dolati P, Sutherland GR. Controversy in the management of lenticulostriate artery dissecting aneurysm: a case report and review of the literature. World neurosurgery. 2014 Feb:81(2):441.e1-7. doi: 10.1016/j.wneu.2012.12.006. Epub 2012 Dec 12 [PubMed PMID: 23246740]
Level 3 (low-level) evidenceOgata A, Sakata S, Okamoto H, Abe T. Ruptured dissecting aneurysm of the recurrent artery of Heubner: Consideration of pathological findings. Neurology India. 2017 May-Jun:65(3):623-625. doi: 10.4103/neuroindia.NI_1034_16. Epub [PubMed PMID: 28488631]
Saito A, Kon H, Nakamura T, Sasaki T. A Dissecting Aneurysm of the Distal Medial Lenticulostriate Artery: Case Report. World neurosurgery. 2016 May:89():725.e1-4. doi: 10.1016/j.wneu.2015.11.066. Epub 2015 Dec 15 [PubMed PMID: 26704207]
Level 3 (low-level) evidenceScott RM, Smith ER. Moyamoya disease and moyamoya syndrome. The New England journal of medicine. 2009 Mar 19:360(12):1226-37. doi: 10.1056/NEJMra0804622. Epub [PubMed PMID: 19297575]
Takekawa Y, Umezawa T, Ueno Y, Sawada T, Kobayashi M. Pathological and immunohistochemical findings of an autopsy case of adult moyamoya disease. Neuropathology : official journal of the Japanese Society of Neuropathology. 2004 Sep:24(3):236-42 [PubMed PMID: 15484702]
Level 3 (low-level) evidenceLin R, Xie Z, Zhang J, Xu H, Su H, Tan X, Tian D, Su M. Clinical and immunopathological features of Moyamoya disease. PloS one. 2012:7(4):e36386. doi: 10.1371/journal.pone.0036386. Epub 2012 Apr 27 [PubMed PMID: 22558457]
Komiyama M. Moyamoya Disease is a Progressive Occlusive Arteriopathy of the Primitive Internal Carotid Artery. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2003 Mar 30:9(1):39-45 [PubMed PMID: 20591301]
Takahashi M. Magnification angiography in moyamoya disease: new observations on collateral vessels. Radiology. 1980 Aug:136(2):379-86 [PubMed PMID: 7403514]
Kronenburg A, Braun KP, van der Zwan A, Klijn CJ. Recent advances in moyamoya disease: pathophysiology and treatment. Current neurology and neuroscience reports. 2014 Jan:14(1):423. doi: 10.1007/s11910-013-0423-7. Epub [PubMed PMID: 24310442]
Level 3 (low-level) evidenceHuang S, Guo ZN, Shi M, Yang Y, Rao M. Etiology and pathogenesis of Moyamoya Disease: An update on disease prevalence. International journal of stroke : official journal of the International Stroke Society. 2017 Apr:12(3):246-253. doi: 10.1177/1747493017694393. Epub 2017 Jan 1 [PubMed PMID: 28381201]
Arias EJ, Derdeyn CP, Dacey RG Jr, Zipfel GJ. Advances and surgical considerations in the treatment of moyamoya disease. Neurosurgery. 2014 Feb:74 Suppl 1():S116-25. doi: 10.1227/NEU.0000000000000229. Epub [PubMed PMID: 24402480]
Level 3 (low-level) evidenceArboix A, Martí-Vilalta JL. Lacunar stroke. Expert review of neurotherapeutics. 2009 Feb:9(2):179-96. doi: 10.1586/14737175.9.2.179. Epub [PubMed PMID: 19210194]
Venkataraman P, Tadi P, Lui F. Lacunar Syndromes (Archived). StatPearls. 2025 Jan:(): [PubMed PMID: 30480945]
Lammie GA. Pathology of small vessel stroke. British medical bulletin. 2000:56(2):296-306 [PubMed PMID: 11092081]
Decavel P, Vuillier F, Moulin T. Lenticulostriate infarction. Frontiers of neurology and neuroscience. 2012:30():115-9. doi: 10.1159/000333606. Epub 2012 Feb 14 [PubMed PMID: 22377876]