Introduction
Sebaceous gland hyperplasia (SGH) is a benign and common condition of sebaceous glands.
SGH affects adults of middle age or older, mainly males. It reportedly occurs in approximately 1% of the healthy population. Sebaceous hyperplasia is not rare in newborns: an Iranian prospective cohort study reported that 43.7% of 1000 consecutive neonates examined had sebaceous hyperplasia; its appearance in that situation is transient and results from exposure to maternal hormones.[1][2] It is uncommon during childhood and adolescence.[3] It has been described in patients on chronic immunosuppressive therapy: reports of the prevalence of SGH are as high as 10 to 16% in patients treated for long-period with cyclosporine A.[4] It has also been associated with genetic syndromes, in rare cases of Muir-Torre.[5] In general, sebaceous adenomas more strongly correlate with that syndrome, and sebaceous hyperplasias are common in patients without any underlying condition.
Sebaceous glands have acini attached to an excretory duct; the production of sebum occurs inside the sebocyte, which accumulates lipids during its life cycle and then releases its content inside the principal excretory duct. Sebaceous glands are androgen-sensitive, so their activity differs according to circulating hormone levels and age. Sebaceous hyperplasia is composed of normally-looking glands with an increased number of acini and mature sebocytes.
The primary differential diagnoses include sebaceous adenoma, nevus sebaceus, lupus miliaris disseminatus faciei, and basal cell carcinoma.
Treatment for sebaceous hyperplasia is usually not needed but can merit consideration when it becomes a cosmetic issue or if it is clinically confused with a more concerning lesion. Various treatments are available for this condition, including cryotherapy or cryosurgery, photodynamic therapy, laser treatment (argon, carbon dioxide, or pulsed-dye laser), cauterization, or electrodesiccation shaving or excision, topical treatments with chloroacetic or trichloroacetic acid, and systemic treatment with isotretinoin.[6][7][8][9][10]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Sebaceous hyperplasia is a benign disease and generally does not require treatment. However, lesions can be unsightly and bothersome. The main concern is the clinical resemblance with other neoplastic lesions such as sebaceous adenoma and basal cell carcinoma.
Causes
Sebaceous glands are highly sensitive to circulating androgens and have specific androgen-converting enzymes. The pathogenesis surrounding SGH involves the changing hormonal environment that comes with increasing age. In men, this often occurs in the eighth decade of life, while in women, it happens shortly after menopause. Decreasing levels of androgens lead to a decrease in sebocyte turnover, which activates a feedback stimulation of sebocyte proliferation within the gland and sebaceous hyperplasia. The effect is most pronounced over the face. The hormonal influence of insulin, TSH, and hydrocortisone also increase sebocyte proliferation.
Sebaceous hyperplasia has been linked to long-term treatment with cyclosporine in the setting of organ transplantation, and specifically with the lipophilic cyclosporine A, due to a stimulatory effect on undifferentiated sebocytes.[11][4] Levandoski reported a case of sebaceous hyperplasia in a renal transplant patient without prior exposure to cyclosporine, treated with the immunosuppressant tacrolimus.
Sebaceous hyperplasia has been documented as a side effect of HIV antiretroviral treatment.[12]
Although SGH is common in the older population, presenile diffuse familial sebaceous hyperplasia (PDFSH) cases have been reported in the literature.[13] This form of sebaceous hyperplasia is linked to a genetic predisposition, has an earlier age of onset, and does not involve the periorificial regions.[14]
Anatomical Pathology
Sebaceous glands are skin appendages found in all parts of the body except on the soles and palms. The areas where there is the highest concentration of sebaceous glands are the face, back, upper arms, and chest. Sebaceous glands are composed of holocrine acini attached to a common excretory duct and a follicle, and together they comprise the pilosebaceous unit. Special types of sebaceous glands are not linked to the pilosebaceous unit and open directly towards the epithelial surface: in lips and buccal mucosa (Fordyce spots), glans penis or clitoris (Tyson glands), areolae (Montgomery's glands), and eyelids (Meibomian glands).
The cells that form the sebaceous gland are called sebocytes and are organized in layers inside the acini. In the basal layer, there are reservoir cells (germinative cells) with basophilic nuclei: that's the mitotically active part of the gland. As sebocytes differentiate, they accumulate increasing amounts of lipids inside the cytoplasm and migrate toward the central excretory duct. The mature sebocytes have vacuolated cytoplasms and small central nuclei with a scalloping effect due to compression by their lipid content. They are present near the central duct, and they disintegrate at the end of their life cycle, releasing their content (lipid and cellular debris) as sebum. The turnover time from sebocyte production to disintegration is approximately 1 month.
Sebocytes arise in the fetus at 13 weeks from the outer root sheath of hair follicles. In the fetus at term, the effect of transplacental maternal androgens results in highly active sebaceous glands, responsible for the production of a protective layer called vernix caseosa. Their activity and size regress in the newborn due to the withdrawal of maternal hormones. Sebaceous production is minimal throughout infancy and childhood. At puberty, as androgen production increases, sebaceous glands enlarge and become increasingly active, peaking during the third decade of life. In older adults, androgen levels decrease, and the sebum production slows down.[15] The decreasing levels of androgens result in smaller sebocytes with lower lipid content and larger nuclei; those sebocytes migrate slowly through the sebaceous gland. As migration of the sebocytes slows, the gland and the sebaceous duct become enlarged with increased basal cells.
In SGH, the sebaceous glands are normal in structure but increased in number. The acini are attached to the central duct, which may become dilated. The presence of four or more sebaceous lobules around a hair follicle has been suggested as a diagnostic clue. Sebaceous lobules show increasing numbers and slightly in size, are located in a more superficial position in the dermis, and have only two layers of germinative cells.
The differential diagnosis primarily includes sebaceous adenoma. Adenoma has an increased number of germinative cells (more than two layers) and the presence of immature eosinophilic sebocytes. There are architectural abnormalities, including the displacement of normal epithelial structures replaced by sebaceous elements. Mature sebocytes comprise more than 50% of the lesion.
Sebaceoma is another entity that can cause clinical confusion with sebaceous hyperplasia. It is a circumscribed and symmetrical lesion composed of solid nodules of immature sebocytes and germinative cells, duct-like spaces, and cystic changes. The germinative cells form the main part of the lesion, representing more than 50% of the cells. The overlying epidermis can appear keratotic, crusted, or ulcerated.
Superficial epithelioma with sebaceous differentiation or reticulated acanthoma with sebaceous differentiation (RASD) is a rare entity initially proposed by Steffen and Ackerman.[16][17][18] There is epidermal acanthosis associated with clusters of sebocytes in a pattern that resembles reticulated seborrheic keratosis. The epidermis shows a superficial reticulated proliferation of keratinocytes, and the sebocytes are mature with a thin layer of germinative cells surrounding the lobules.
Nevus sebaceus (spelling is correct without the "o" normally found in the word sebaceous) is a common hamartoma typically present at birth or appear during early childhood in the head and neck region. Histology shows papillomatosis and hyperkeratosis, prominent sebaceous hyperplasia with the absence of hair follicles. Apocrine glands are often present. Sebaceous glands are abnormal in morphology and distribution: the localization is high within the dermis, and the ducts communicate directly with the epidermal surface.
Basal cell carcinoma (BCC) can be clinically similar to sebaceous hyperplasia, particularly in solitary lesions of sun-exposed areas of the face. BCC shows basaloid proliferation of neoplastic cells with peripheral palisading, tumor stromal-clefting, and extracellular mucin features not present in sebaceous neoplasms.
Although sebaceous differentiation is evident in most cases of benign sebaceous neoplasms, special stains may be required. Epithelial membrane antigen (EMA) expresses in the cytoplasm in up to 100% of cases.[15] Cytokeratin (CK) 7 and androgen receptor (AR) are also often expressed, but stains for these three antigens are not specific for sebaceous neoplasms because they can express in other adnexal tumors. Oil-Red-O (a lipid stain) can be performed, but requires a frozen section, and is not possible on the usual formalin-fixed, paraffin-embedded sections. More specific stains are adipophilin and Factor XIIIa (AC-1A1 clone).[19][20]
Given the association of sebaceous adenomas (and only rarely sebaceous hyperplasias) with Muir-Torre syndrome, stains to detect a clinically-undiagnosed microsatellite instability are options. Diagnosis of this syndrome could potentially help to help detect visceral neoplasms (especially colon cancer) at their pre-clinical stage, improving survival, but this is not something to consider with the usual example of sebaceous gland hyperplasia.
Clinical Pathology
No laboratory studies are necessary. Sebaceous hyperplasia is diagnosed based on clinical examination or assisted by dermoscopy. A biopsy can be appropriate in differential diagnosis with basal cell carcinoma. Histopathological examination of sebaceous hyperplasia lesions reveals enlarged glands with normal morphology. Inside each gland, mature sebaceous lobules connect to a dilated principal sebaceous duct.
Biochemical and Genetic Pathology
Sebum production, together with sweat production, is highly androgen-sensitive; the activity and size of sebaceous glands are different according to age and circulating hormone levels. The number of sebaceous gland units remains approximately the same throughout life, but their metabolic rate differs during different life stages. Sebocytes contain androgen-metabolizing enzymes (5-alpha-reductase type I, 3-beta-hydroxysteroid dehydrogenase, 17-beta-hydroxysteroid dehydrogenase type II) which metabolize weak circulating androgens into potent androgens; a typical conversion is dehydroepiandrosterone-sulfate into dihydrotestosterone. The latter binding to androgen-specific receptors of the sebocytes increases their size and metabolic rate. Scalp and face are areas where the 5-alpha-reductase has the highest activity in conversion towards testosterone and dihydrotestosterone, stimulating sebaceous gland proliferation. The opposite effect occurred for estrogens, which decrease sebaceous gland activity.
Although SGH etiology has shown links to both intrinsic and extrinsic factors, the principal genetic changes remain unknown. Leopold et al. support the hypothesis that mutations in the EGFR-RASMAPK pathway play an important role in the pathogenesis of SGH.[21]
Sebaceous hyperplasia occasionally occurs in areas of the body without UV exposure, including the buccal mucosa, vulva, and areolae; otherwise, UV rays are considered as a cofactor.[22][23][24]
Muir–Torre syndrome (MTS), described by Muir et al. in 1967 and Torre in 1968, is characterized by the presence of both sebaceous neoplasms and visceral malignancies.[25] The association with sebaceous hyperplasia is controversial, but research has demonstrated it in some cases; MTS should be a consideration in the appropriate clinical setting.[26][27][28][29][30] The transmission is typically autosomal dominant, so the identification of one patient can potentially aid in the identification of multiple cases in the entire family. It is considered a variant of hereditary non-polyposis colorectal cancer (HNPCC) syndrome.[31]
The presence of germ-line mutations in DNA mismatch repair genes affects the proteins MLH1 or MSH2 and the microsatellite instability complex. About 35% of the cases are microsatellite stable, some associated with biallelic inactivation of MYH. Loss of the mismatch repair complex can be demonstrated by immunohistochemistry against MLH1, MSH2, MSH6, and PMS2. Loss of MSH2 and MSH6 staining is the most common pattern (63% of cases). Loss of the proteins MLH1 and PMS2 accounts for 19% of cases, while MSH6 loss accounts for the other 15% of cases. It is crucial to consider the cost-effectiveness of the test and its ethical implications. Also, identification of somatic mutation is more important than finding a germ-line mutation in individual lesions, because germ-line mutations can occur within lesions, without patients having MTS.
Morphology
SGH lesions can be isolated or multiple, present mainly on the face or less frequently on other parts of the body as soft yellow papules. On physical examination, the papules show a central umbilication and branching vessels, especially if examined using a dermatoscope. A biopsy may be necessary to rule out basal cell carcinoma.[32][11] However, papules of sebaceous hyperplasia are typically multiple and yellowish and are observable as small lobules with the aid of magnification dermoscopy.
Rare variants of SGH include a linear form, zosteriform arrangement, a diffuse form, a giant form, a nevoid form, and a familial form.[33][34][35]
Clinicopathologic Correlations
The classical clinical presentation of SGH is of a solitary nodule or multiple skin-colored or yellowish papules localized on the face (forehead, cheeks, chin) or in the upper trunk. The clinical lesions display a central dell corresponding to the follicular infundibular ostium. These lesions are soft and vary in size from 2 to 9 mm.
Dermoscopically, sebaceous hyperplasia reveals a pattern composed of aggregated white-yellowish nodules corresponding to hyperplastic sebaceous glands. The ostium of the gland is sometimes visible as a small crater or umbilication in the center of those yellowish nodules.[36] Surrounding the nodules, there is a vascular pattern visible with dermoscopy; the most common and specific is the so-called "crown vessels", which may extend toward the center without crossing it. The dermoscopic findings significantly aid in the diagnosis.[37]
Clinical Significance
These lesions are benign but can create a cosmetic concern. They are challenging to treat; the entire sebaceous unit must be eliminated to prevent a recurrence. The severity of SGH lesions has been classified as limited if less than ten lesions are recognized, moderate (10 to 50 lesions), frequent (less than 100 lesions), and very frequent (more than 100 lesions).[38]
Sebaceous hyperplasia is treatable with different techniques with variable cosmetic results. The therapeutic outcomes have been categorized as optimal (if results in no scarring and no hypo- or hyperpigmentation), moderate (moderate scarring and/or hypo- or hyperpigmentation), and poor (scarring and/or hypo- or hyperpigmentation is prominent).
The main treatments are pharmaceutical agents like trichloroacetic acid (topic treatment) and isotretinoin (systemic). Physical treatments are cryotherapy, electrodesiccation, photodynamic and laser therapy, excision, shave, and curettage. Cryotherapy, electrodesiccation, curettage, excision, and topical trichloroacetic acid can cause skin discoloration and scarring so that the cosmetic outcome can be unsatisfactory. Photodynamic therapy uses with the wavelength of 1720 nm that is said to be specific for the sebaceous gland unit; it provides minimal damage to the surrounding tissues but requires multiple sessions and special equipment.[39] The most appropriate lasers used to treat SGH are Argon and carbon dioxide (CO2). Oral isotretinoin is effective, but the treatment must continue for several months, and there are high relapse rates with discontinuation. It is not for use during pregnancy.
Media
(Click Image to Enlarge)
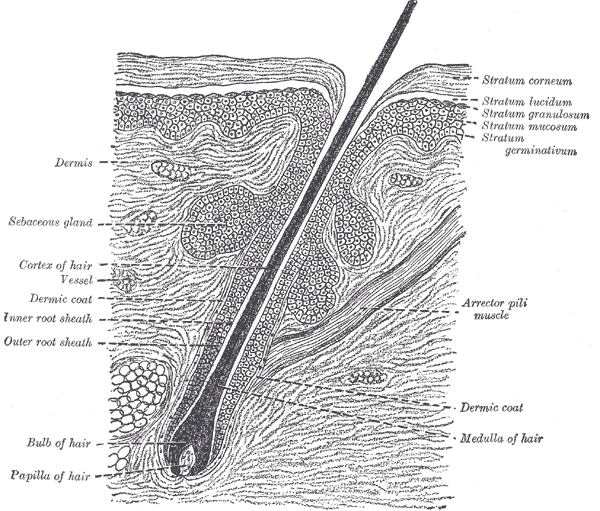
The Common Integument, Section of the Skin. A section of the skin showing the epidermis, dermis, hair shaft and follicle, arrector pili muscles, and sebaceous glands.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Multiple sebaceous hyperplasias on forehead. These regressed with oral isotretinoin treatment. Contributed by Ronald Rapini, MD
(Click Image to Enlarge)

Pilosebaceous unit. The hair shaft (H) is present within the follicle. The sebaceous glands (S) connect to the follicle at its mid-portion, where there is an eosinophilic cuticle lining (C). Contributed by Ronald Rapini MD
(Click Image to Enlarge)
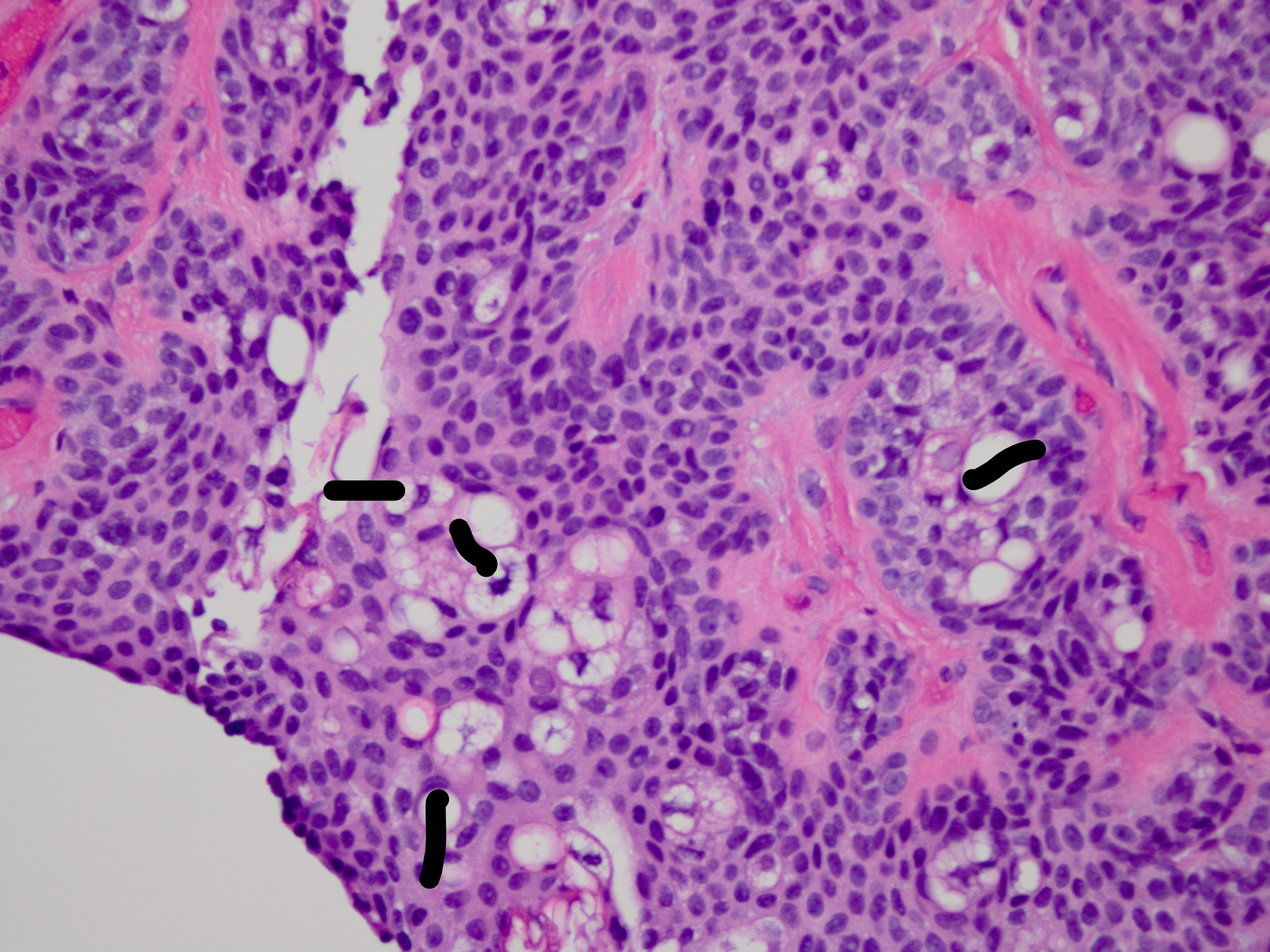
Sebocytes have a soap bubble appearance. Their nuclei are scalloped or indented (black marks). Contributed by Ronald Rapini, MD.
(Click Image to Enlarge)
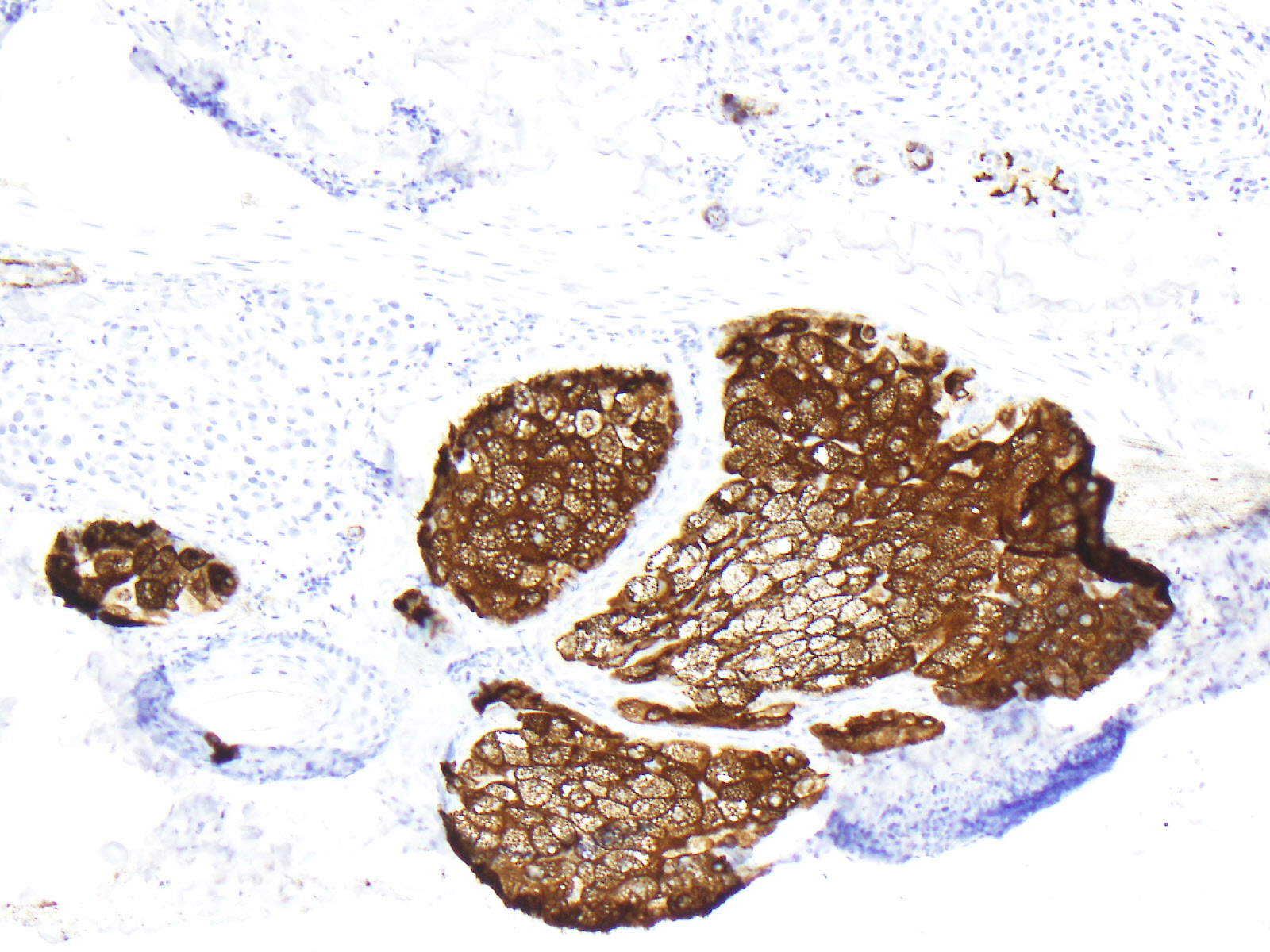
Sebaceous glands stained for EMA (epithelial membrane antigen). Contributed by Ronald Rapini, MD.
References
Kanada KN, Merin MR, Munden A, Friedlander SF. A prospective study of cutaneous findings in newborns in the United States: correlation with race, ethnicity, and gestational status using updated classification and nomenclature. The Journal of pediatrics. 2012 Aug:161(2):240-5. doi: 10.1016/j.jpeds.2012.02.052. Epub 2012 Apr 11 [PubMed PMID: 22497908]
Moosavi Z, Hosseini T. One-year survey of cutaneous lesions in 1000 consecutive Iranian newborns. Pediatric dermatology. 2006 Jan-Feb:23(1):61-3 [PubMed PMID: 16445415]
Level 2 (mid-level) evidenceIreland AM, Harvey NT, Berry BD, Wood BA. Paediatric cutaneous adnexal tumours: a study of 559 cases. Pathology. 2017 Jan:49(1):50-54. doi: 10.1016/j.pathol.2016.10.003. Epub 2016 Nov 30 [PubMed PMID: 27914683]
Level 3 (low-level) evidenceBoschnakow A, May T, Assaf C, Tebbe B, Zouboulis ChC. Ciclosporin A-induced sebaceous gland hyperplasia. The British journal of dermatology. 2003 Jul:149(1):198-200 [PubMed PMID: 12890221]
Level 3 (low-level) evidenceRosenfield RL, Deplewski D, Greene ME. Peroxisome proliferator-activated receptors and skin development. Hormone research. 2000:54(5-6):269-74 [PubMed PMID: 11595816]
Level 3 (low-level) evidenceAtaş H, Gönül M. Evaluation of the Efficacy of Cryosurgery in Patients With Sebaceous Hyperplasia of the Face. Journal of cutaneous medicine and surgery. 2017 May/Jun:21(3):202-206. doi: 10.1177/1203475416685076. Epub 2016 Dec 27 [PubMed PMID: 28300439]
Horio T, Horio O, Miyauchi-Hashimoto H, Ohnuki M, Isei T. Photodynamic therapy of sebaceous hyperplasia with topical 5-aminolaevulinic acid and slide projector. The British journal of dermatology. 2003 Jun:148(6):1274-6 [PubMed PMID: 12828768]
Level 3 (low-level) evidenceAghassi D, González E, Anderson RR, Rajadhyaksha M, González S. Elucidating the pulsed-dye laser treatment of sebaceous hyperplasia in vivo with real-time confocal scanning laser microscopy. Journal of the American Academy of Dermatology. 2000 Jul:43(1 Pt 1):49-53 [PubMed PMID: 10863223]
Bader RS, Scarborough DA. Surgical pearl: intralesional electrodesiccation of sebaceous hyperplasia. Journal of the American Academy of Dermatology. 2000 Jan:42(1 Pt 1):127-8 [PubMed PMID: 10607331]
Rosian R, Goslen JB, Brodell RT. The treatment of benign sebaceous hyperplasia with the topical application of bichloracetic acid. The Journal of dermatologic surgery and oncology. 1991 Nov:17(11):876-9 [PubMed PMID: 1757649]
de Berker DA, Taylor AE, Quinn AG, Simpson NB. Sebaceous hyperplasia in organ transplant recipients: shared aspects of hyperplastic and dysplastic processes? Journal of the American Academy of Dermatology. 1996 Nov:35(5 Pt 1):696-9 [PubMed PMID: 8912563]
Short KA, Williams A, Creamer D, Fuller LC. Sebaceous gland hyperplasia, human immunodeficiency virus and highly active anti-retroviral therapy. Clinical and experimental dermatology. 2008 May:33(3):354-5. doi: 10.1111/j.1365-2230.2007.02670.x. Epub 2008 Mar 16 [PubMed PMID: 18346183]
Level 3 (low-level) evidenceLiu YS, Cheng YP, Liu CI, Yang CY, Yang CY. Presenile diffuse familial sebaceous hyperplasia successfully treated with low-dose isotretinoin: A report of two cases and review of the published work. The Journal of dermatology. 2016 Oct:43(10):1205-1208. doi: 10.1111/1346-8138.13416. Epub [PubMed PMID: 27130181]
Level 3 (low-level) evidenceDupre A, Bonafe JL, Lamon P. Functional familial sebaceous hyperplasia of the face and premature sebaceous gland hyperplasia: a new and unique entity. Journal of the American Academy of Dermatology. 1983 Nov:9(5):768-9 [PubMed PMID: 6643776]
Level 3 (low-level) evidenceIacobelli J, Harvey NT, Wood BA. Sebaceous lesions of the skin. Pathology. 2017 Dec:49(7):688-697. doi: 10.1016/j.pathol.2017.08.012. Epub 2017 Oct 25 [PubMed PMID: 29078997]
Coelho A, Luzar B. Superficial epithelioma with sebaceous differentiation: a case report with literature review. Acta dermatovenerologica Alpina, Pannonica, et Adriatica. 2017 Sep:26(3):63-66 [PubMed PMID: 28941264]
Level 3 (low-level) evidenceIto T, Yoshida Y, Furue M, Yamamoto O. Dermoscopic features of reticulated acanthoma (superficial epithelioma) with sebaceous differentiation. European journal of dermatology : EJD. 2012 Sep-Oct:22(5):704-6. doi: 10.1684/ejd.2012.1807. Epub [PubMed PMID: 22858895]
Level 3 (low-level) evidenceFriedman KJ, Boudreau S, Farmer ER. Superficial epithelioma with sebaceous differentiation. Journal of cutaneous pathology. 1987 Aug:14(4):193-7 [PubMed PMID: 3305610]
Ostler DA, Prieto VG, Reed JA, Deavers MT, Lazar AJ, Ivan D. Adipophilin expression in sebaceous tumors and other cutaneous lesions with clear cell histology: an immunohistochemical study of 117 cases. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2010 Apr:23(4):567-73. doi: 10.1038/modpathol.2010.1. Epub 2010 Jan 29 [PubMed PMID: 20118912]
Level 3 (low-level) evidenceUhlenhake EE, Clark LN, Smoller BR, Shalin SC, Gardner JM. Nuclear factor XIIIa staining (clone AC-1A1 mouse monoclonal) is a sensitive and specific marker to discriminate sebaceous proliferations from other cutaneous clear cell neoplasms. Journal of cutaneous pathology. 2016 Aug:43(8):649-56. doi: 10.1111/cup.12726. Epub 2016 Jun 10 [PubMed PMID: 27153339]
Groesser L, Singer S, Peterhof E, Landthaler M, Heigl U, Schneider-Brachert W, Berneburg M, Hafner C. KRAS, HRAS and EGFR Mutations in Sporadic Sebaceous Gland Hyperplasia. Acta dermato-venereologica. 2016 Aug 23:96(6):737-41. doi: 10.2340/00015555-2351. Epub [PubMed PMID: 26804118]
Daley TD. Intraoral sebaceous hyperplasia. Diagnostic criteria. Oral surgery, oral medicine, and oral pathology. 1993 Mar:75(3):343-7 [PubMed PMID: 8469546]
Malliah R, Gilhooly P, Lambert WC, Heller DS. Sebaceous hyperplasia of the vulva: case report and review of the literature. Journal of lower genital tract disease. 2006 Jan:10(1):55-7 [PubMed PMID: 16378033]
Level 3 (low-level) evidenceChiriac A, Moldovan C, Coros MF, Podoleanu C, Moncea D, Stolnicu S. Bilateral areolar sebaceous hyperplasia in a post-menopausal woman. European journal of dermatology : EJD. 2016 Jun 1:26(3):299-300. doi: 10.1684/ejd.2016.2739. Epub [PubMed PMID: 27032720]
Torre D. Multiple sebaceous tumors. Archives of dermatology. 1968 Nov:98(5):549-51 [PubMed PMID: 5684233]
Level 3 (low-level) evidenceJakobiec FA, Cortes Barrantes P, Milman T, Lee NG, Fay A. Ocular Adnexal Adenomatoid Sebaceous Gland Hyperplasia: A Clinical and Immunopathologic Analysis in Relation to the Muir-Torre Syndrome. Ophthalmic plastic and reconstructive surgery. 2020 Jan/Feb:36(1):e6-e12. doi: 10.1097/IOP.0000000000001497. Epub [PubMed PMID: 31593035]
Roma AA, Barry J, Pai RK, Billings SD. Sebaceous hyperplasia of the vulva: a series of cases reporting no association with the Muir-Torre syndrome. International journal of gynecological pathology : official journal of the International Society of Gynecological Pathologists. 2014 Jul:33(4):437-42. doi: 10.1097/PGP.0b013e31829ff21e. Epub [PubMed PMID: 24901406]
Level 3 (low-level) evidenceKruse R, Rütten A, Schweiger N, Jakob E, Mathiak M, Propping P, Mangold E, Bisceglia M, Ruzicka T. Frequency of microsatellite instability in unselected sebaceous gland neoplasias and hyperplasias. The Journal of investigative dermatology. 2003 May:120(5):858-64 [PubMed PMID: 12713593]
Ponti G, Meschieri A, Pollio A, Ruini C, Manfredini M, Longo C, Mandel VD, Ciardo S, Tomasi A, Giannetti L, Pellacani G. Fordyce granules and hyperplastic mucosal sebaceous glands as distinctive stigmata in Muir-Torre syndrome patients: characterization with reflectance confocal microscopy. Journal of oral pathology & medicine : official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology. 2015 Aug:44(7):552-7. doi: 10.1111/jop.12256. Epub 2014 Sep 12 [PubMed PMID: 25213213]
Spraul CW, Jakobczyk-Zmija MJ, Lang GK. [Sebaceous hyperplasia of the lower eyelid]. Klinische Monatsblatter fur Augenheilkunde. 1999 Nov:215(5):319-20 [PubMed PMID: 10609249]
Level 3 (low-level) evidenceJohn AM, Schwartz RA. Muir-Torre syndrome (MTS): An update and approach to diagnosis and management. Journal of the American Academy of Dermatology. 2016 Mar:74(3):558-66. doi: 10.1016/j.jaad.2015.09.074. Epub [PubMed PMID: 26892655]
Salim A, Reece SM, Smith AG, Harrison D, Ramsay HM, Harden PN, Fryer AA. Sebaceous hyperplasia and skin cancer in patients undergoing renal transplant. Journal of the American Academy of Dermatology. 2006 Nov:55(5):878-81 [PubMed PMID: 17052497]
Level 2 (mid-level) evidenceSato T, Tanaka M. Linear sebaceous hyperplasia on the chest. Dermatology practical & conceptual. 2014 Jan:4(1):93-5. doi: 10.5826/dpc.0401a16. Epub 2014 Jan 31 [PubMed PMID: 24520522]
Level 3 (low-level) evidenceKato N, Yasuoka A. "Giant" senile sebaceous hyperplasia. The Journal of dermatology. 1992 Apr:19(4):238-41 [PubMed PMID: 1607487]
Level 3 (low-level) evidenceMandal RK, Das A, Chakrabarti I, Agarwal P. Nevoid sebaceous hyperplasia mistaken as nevus sebaceous: Report of four cases. Indian journal of dermatology, venereology and leprology. 2017 Mar-Apr:83(2):213-216. doi: 10.4103/0378-6323.199424. Epub [PubMed PMID: 28164886]
Level 3 (low-level) evidenceZaballos P, Gómez-Martín I, Martin JM, Bañuls J. Dermoscopy of Adnexal Tumors. Dermatologic clinics. 2018 Oct:36(4):397-412. doi: 10.1016/j.det.2018.05.007. Epub 2018 Aug 16 [PubMed PMID: 30201149]
Kim NH, Zell DS, Kolm I, Oliviero M, Rabinovitz HS. The dermoscopic differential diagnosis of yellow lobularlike structures. Archives of dermatology. 2008 Jul:144(7):962. doi: 10.1001/archderm.144.7.962. Epub [PubMed PMID: 18645159]
Level 3 (low-level) evidenceKavoussi H, Rezaei M, Azimi M, Kavoussi R. Combination of CO2 laser therapy and curettage for sebaceous gland hyperplasia. Acta dermatovenerologica Alpina, Pannonica, et Adriatica. 2019 Mar:28(1):11-14 [PubMed PMID: 30901063]
Simmons BJ, Griffith RD, Falto-Aizpurua LA, Bray FN, Nouri K, International League of Dermatological Societies, European Dermatology Forum. Light and laser therapies for the treatment of sebaceous gland hyperplasia a review of the literature. Journal of the European Academy of Dermatology and Venereology : JEADV. 2015 Nov:29(11):2080-7. doi: 10.1111/jdv.13066. Epub 2015 Mar 2 [PubMed PMID: 25731611]
Level 1 (high-level) evidence