Introduction
Trachoma is a debilitating eye disease caused by the Chlamydia trachomatis bacterium and is one of the leading causes of blindness worldwide.[1][2] If left untreated, this bacterial illness primarily affects the conjunctiva, leading to recurrent cycles of inflammation, roughening, and scarring of the inner surface of the eyelids, as well as erosion of the corneal surface. These ocular complications often result in permanent blindness. The World Health Organization (WHO) has classified 20 illnesses and disease groupings as neglected tropical diseases, including trachoma, which is considered the most frequent infection that causes visual impairment in underprivileged countries.[3]
As living standards have improved, trachoma has declined significantly in most North American and European countries.[4] Sharp reductions in the worldwide burden of the disease have been attributed to intentional management measures implemented over the past few decades.[5] However, despite prolonged and intensive interventions, the prevalence of trachoma persists in certain cultures.
Stages of Trachoma
Trachoma manifests in 2 distinct stages, each presenting unique symptoms and complications.
First-phase symptoms: These symptoms include persistent keratoconjunctivitis characterized by inflammation of the conjunctiva, known as active trachoma.[6] This inflammation results from recurrent infections with conjunctival strains of the bacterium C trachomatis.
Second-phase symptoms: The progression to the second stage of the illness is marked by periods of intense conjunctival inflammation, leading to eyelid scarring. Trichiasis is a disorder in which the eyelashes rotate inward and come in touch with the eyeball due to scarring.[7] In addition, a condition called entropion can occur concurrently with trichiasis, where a portion or all of the eyelid edge curls inward.[8] Inverted eyelashes that scratch the cornea increase the risk of corneal opacity and visual problems, leading to blindness in severe chronic conditions.[9] Any of these pathological processes or clinical manifestations induced by C trachomatis indicate the presence of trachoma (see Image. Eye Disorders and Trachoma-Associated Symptoms).
In addition, it is essential to understand how trachoma is transmitted to implement preventative measures. Trachoma mainly spreads through direct and indirect contact with secretions from the noses and eyes of infected individuals. Additionally, transmission can occur through direct contact, hand-eye contact, contact with contaminated objects (fomites), and eye-seeking flies. Several factors contribute to the spread of trachoma, including crowded living conditions, poor hygiene practices, and limited access to medical care. Additionally, socioeconomic status, climate, and cultural customs play significant roles in the transmission of the disease. These factors, often referred to as the "3 F's" in studies, contribute to its dissemination among populations:[10]
- Face-to-face contact: Close contact facilitates the rapid transmission of the highly infectious trachoma disease. This often happens through actions such as kissing, embracing, or sharing intimate objects such as towels and washcloths with an affected individual.[11] During such interactions, the exchange of infected nasal and ocular secretions between individuals can easily spread the bacteria from one person to another.
- Flies: Flies, particularly species such as Musca sorbens, have a significant role in the transmission of trachoma.[12] These flies are attracted to the secretions from people's noses and eyes and act as mechanical vectors by carrying the bacteria on their bodies. Subsequently, they transfer the infection from one person to another. This mode of transmission is especially common in unsanitary environments where flies are plentiful.
- Fomites: Fomites, such as contaminated inanimate objects or surfaces, also contribute to the spread of the bacteria.[13] Infected individuals can transfer the bacterium to items such as linens, towels, or everyday utensils. Those who subsequently come into contact with these contaminated fomites and then touch their face or eyes are at risk of contracting the bacteria.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The causative agent of trachoma, the C trachomatis bacterium, is transmitted from infected to uninfected individuals through various means, including direct eye-to-eye spread during close contact, hand-eye contact, indirect transmission via contaminated objects (fomites), and transmission facilitated by eye-seeking flies.[14] Several factors, including crowded living arrangements, poor hygiene habits, and restricted access to sanitary facilities and clean water, contribute to the spread of trachoma.[15] These conditions create an environment conducive to the growth and persistence of C trachomatis bacteria within communities, continuing the infection cycle. Understanding the root causes of trachoma is crucial for developing targeted measures to stop the disease's spread, address ongoing infections, and mitigate its long-term impact.
C trachomatis can cause ocular infections such as trachoma and infections transmitted through sexual activity in humans.[16] Trachoma primarily affects the conjunctiva. The interaction between the life cycle of bacteria and the host's immune system plays a crucial role in the development of trachoma. Upon entering the eye, C trachomatis initiates the infection by entering the epithelial cells of the conjunctiva and undergoes a biphasic developmental cycle. The infectious form of the bacteria, known as the elementary bodies, initially binds to and penetrates the host cells.[17] Subsequently, once inside, they undergo differentiation into reticulate bodies, which multiply within the host cell's cytoplasm.[18]
The typical clinical signs of trachoma, such as conjunctival inflammation, follicular enlargement, and eventual scarring of the eyelids, are caused by the localized inflammatory response elicited by the replication of reticulate bodies.[19] The pathophysiology and regulation of trachoma are significantly influenced by the immunological response triggered by the infection. Although an effective immune response can facilitate the clearance of the infection, recurrent or persistent infections may lead to chronic inflammation and scarring, resulting in long-term complications such as trichiasis and blindness.[20]
Epidemiology
Trachoma ranks as the third leading cause of blindness globally, following cataracts and glaucoma.[21] According to estimates, nearly 8 million people are either blind or suffer from severe visual impairment due to trachoma.[22] The highest prevalence of the disease is observed in regions such as Africa, certain parts of the Middle East, the Indian subcontinent, Southeast Asia, and South America.[23] Studies conducted in June 2021 indicated that nearly 2 million individuals worldwide were on the brink of blindness due to trachoma, with an estimated 137 million people at risk of contracting the disease.[24] Epidemiological surveys conducted in 2023 revealed that around 116 million individuals globally resided in areas that warranted preventative measures for trachoma prevention and elimination. Furthermore, only 18 out of the known 62 trachoma-endemic countries had succeeded in eradicating the disease as a public health concern.[25][26]
Targeted public health measures have significantly reduced the prevalence of trachoma—a disease that was once widespread in many regions of the world. However, it remains a concern in certain areas, particularly in low- and middle-income countries with restricted access to hygienic and medical services. Various factors, including socioeconomic status, geographic location, and cultural practices, influence the epidemiology of trachoma.
Many countries in Africa are still in need of active preventative measures for trachoma.[27] In contrast, North America and Europe have experienced a significant reduction in disease prevalence primarily due to overall improvements in living standards rather than specific interventions.[14] Although the goal of eradicating trachoma worldwide by 2020 has not been achieved, hope remains with the implementation of treatment and prevention programs in endemic regions aiming to achieve the goal of disease elimination by 2030.[28]
Trachoma disproportionately affects women and children.[29] This gender disparity stems from women's increased exposure to contaminated water and unsanitary conditions, often due to their involvement with childcare and household duties.[30] Studies have shown that the odds ratio can be 1.8 to 4 times higher in females than males.[31]
Age is another significant factor influencing the occurrence of trachoma, with children aged 10 or younger bearing the largest burden. Due to their limited ability to practice basic hygiene and their close contact with infected individuals, young children are particularly susceptible to trachoma. During this age period, the prevalence of active trachoma typically peaks before declining during adolescence and adulthood.[32] On the other hand, individuals who experience untreated childhood infections are at risk of long-term complications such as blindness and trichiasis.
Although the prevalence of trachoma has significantly decreased in many parts of the world, it still poses a severe threat to public health in some areas, especially for marginalized groups of populations with little access to sanitary facilities and medical care. Implementing targeted interventions, including promoting facial cleanliness, improving hygiene and sanitation, ensuring access to clean drinking water, providing antibiotic treatment, and controlling fly populations in endemic areas, is crucial to preventing this pervasive and severe ocular disease and optimizing patient outcomes.
Pathophysiology
The pathophysiology of trachoma is characterized by the development of conjunctival scarring, which results from recurrent cycles of tissue repair and inflammation.[33] Extracellular matrix proteins such as collagen and fibronectin are deposited throughout the scarring process, leading to fibrosis and contraction of the conjunctival tissue.[33] Without treatment for this fibrotic scarring, complications such as eyelid entropion (inward turning of the eyelid) and trichiasis (misalignment of the lashes) may occur, potentially resulting in corneal abrasions, ulcerations, and eventual blindness.[34] Bacterial infection, inflammatory reactions, tissue remodeling, and host factors intricately interact in the pathophysiology of trachoma.[35]
Trachoma is primarily associated with infections by serovars A, B, Ba, and C of the C trachomatis bacterium, while serovars D to K are typically linked to adult inclusion conjunctivitis. Other species within the Chlamydiaceae family, such as Chlamydophila psittaci and C pneumoniae, have also been implicated. Trachoma infection progresses through an initial 'active' inflammatory stage, which is more prevalent in preschool children. This stage may be mild and only result in trachomatous conjunctivitis (follicular or papillary), with the presence of papillary hypertrophy characterizing more severe cases.
Recurrent infection triggers a chronic immune response provoked by intermittent chlamydial antigens. This response manifests as a cell-mediated delayed hypersensitivity (type 4) response. The repeated insult from these antigens leads to scarring and other forms of permanent damage. This chronic "cicatricial" stage typically occurs in middle age, with most scarring concentrated on the upper tarsal plate. As this scar tissue contracts, it causes the in-turning of the lid, resulting in entropion, which eventually leads to trichiasis. Entropion is the most common cause of trichiasis in trachoma patients. However, in rare cases, trichiasis may also occur due to aberrant lashes or metaplastic lashes. Ultimately, blinding corneal opacification can develop as a result of these complications.
The obligate intracellular bacterium C trachomatis and the host's immune system interact intricately in the pathophysiology of trachoma, leading to conjunctival scarring, tissue destruction, and increasing inflammation.[36] During the early stages of infection, the conjunctival epithelial cells serve as the site of attachment and invasion for the elementary bodies of C trachomatis. Once inside the host cell, these elementary bodies transform into reticulate bodies, where they multiply within the infected cells' cytoplasm.[18][37] This intracellular multiplication triggers the infiltration of immune cells, such as neutrophils, macrophages, and lymphocytes, into the conjunctival tissue, eliciting an inflammatory response.
The inflammatory cascade triggered by C trachomatis infection releases proinflammatory cytokines and chemokines, which further amplify the immune response and contribute to tissue damage. Chronic inflammation on the conjunctival surface results in the formation of follicles, which are aggregations of lymphocytes, plasma cells, and epithelial cells. These follicles can potentially progress into papillary hypertrophy, characterized by the enlargement and hyperplasia of the conjunctival papillae.[38] Understanding these mechanisms is imperative for developing targeted interventions aimed at halting the progression of the disease and reducing the incidence of blindness caused by trachoma.
Histopathology
Active trachoma is commonly observed in children infected with C trachomatis. Classic findings include a hyperplastic conjunctival epithelium and widespread inflammatory infiltrates comprising B and T lymphocytes, neutrophils, macrophages, and plasma cells.[39] Staining for collagen subtypes reveals a generalized increase in collagen types 1, 3, and 4, along with the deposition of new type 5 fibers.[40] Conversely, adults with scarring exhibit an atrophic conjunctival epithelium and loss of goblet cells.[41] A thick scar consisting of type 5 collagen replaces the loose subepithelial stroma, with these newer fibers tightly adhering to the tarsal plate, leading to distortion. Conjunctival inflammation is often observed in these cases.
The normal conjunctiva undergoes histological and immunological alterations in active trachoma and trachomatous scarring.[38] Goblet cells, responsible for mucin secretion, are dispersed throughout the non-keratinized, stratified epithelium, which typically consists of 3 to 5 cell layers in a normal conjunctiva. This epithelium is covered by the tear film. Deeper within the lamina propria, connective tissue components such as lymphoid cells and blood arteries are present. Inflammation resulting from a C trachomatis infection is characterized by a mixed inflammatory cell infiltration and the presence of telangiectasia in capillaries and small venules.
Within the lamina propria, most of the mass and the core of lymphoid follicles comprise B cells. These follicles also contain T cells, macrophages, and additional B cells.[42] When large enough, lymphoid follicles can be observed in the everted tarsal conjunctivae, causing deformation of the overlaying epithelium. Goblet cells are reduced in the scarred conjunctiva, leading to a decrease in tear film volume and alterations in its composition. The lamina propria exhibits a scar that demonstrates increasingly disordered scarring. Scars may also affect the tarsal plate and extracellular matrix.
The chronic inflammation associated with trachoma progression leads to papillary hypertrophy, characterized by enlarged and hyperplastic conjunctival papillae.[43] These papillae contain increased inflammatory cells, such as lymphocytes and plasma cells, and are coated in a layer of squamous epithelium. Significant collagen deposition can be seen in severe cases, along with fibrosis, scarring, and disruption of normal tissue architecture in the conjunctiva.[44]
Follicular conjunctivitis, characterized by the formation of follicles within the conjunctival tissue, is one of the distinctive histological features of trachoma.[45] Typically, these follicles exhibit a central germinal center surrounded by a mantle of lymphocytes and epithelial cells. Histological examination of trachomatous follicles commonly reveals the presence of germinal centers, lymphocytic infiltration, and hypertrophy of the surrounding epithelium. Additionally, histopathological analysis of trachoma-affected tissues may reveal structural anomalies such as conjunctival scarring, fibrosis, metaplastic alterations, and inflammatory changes. Conjunctival scarring, marked by the replacement of normal tissue architecture with fibrous tissue, can lead to the rupture of the epithelial barrier and loss of goblet cells. Fibrotic alterations may result in complications such as entropion, trichiasis, and other eyelid abnormalities.[46]
Overall, histopathological examination of tissues affected by trachoma provides valuable insights into the underlying mechanisms of disease progression and the structural changes associated with chronic inflammation and scarring. This microscopic analysis helps guide clinical management and therapeutic interventions to prevent further tissue damage and preserve vision in affected individuals.
History and Physical
History
Patients with trachoma typically present with symptoms such as redness, itching, and irritation of the eyes and eyelids, along with eye discharge, eyelid swelling, eye pain, and sensitivity to light (photophobia). Assessing the duration of these symptoms is crucial. When gathering a patient's medical history, healthcare professionals should inquire about symptoms that could indicate trachoma and potential risk factors for the disease. Specifically, a history of travel to endemic regions, such as North Africa, the Middle East, and India, should be obtained. Additionally, if the patient is sexually active, concomitant vaginitis, cervicitis, or urethritis should be ruled out.
Physical Examination
Healthcare professionals should focus on identifying indications of trachoma in the eyes and surrounding structures.[19] Essential elements of the assessment are mentioned below.[47]
- Evaluation of conjunctival follicles: Trachoma often presents with tiny, raised nodules resembling follicles on the conjunctival surface. These follicles may be scattered widely or clustered in the inferior fornix of the eye.
- Examination of the conjunctiva and eyelids: Healthcare providers should check for symptoms of conjunctival inflammation, including redness, swelling, and discharge. They should also check the eyelids for signs of entropion, characterized by inward bending of the eyelid, or trichiasis, which can cause corneal abrasions and vision problems.
- Visual acuity assessment: Healthcare providers should use standard testing tools, such as the Snellen chart or visual acuity cards, to identify any impairment in vision.
- Assessment of conjunctival scarring: Prolonged inflammation in trachoma patients may lead to conjunctival scarring, which is characterized by fibrotic bands, changes in tissue texture, and loss of normal architecture.
- Analysis of corneal integrity: Clinicians should examine the cornea for any signs of opacities, abrasions, or ulcerations. These conditions can result from persistent irritation caused by trichiasis or corneal exposure due to eyelid abnormalities.
- Evaluation of local lymph nodes and preauricular lymph nodes: A palpator can be used to feel any enlargements suggestive of chlamydial infection–related lymphadenopathy.
A comprehensive medical history and physical examination are crucial for the diagnostic evaluation of trachoma. Identifying distinctive indications and risk variables for the ailment can direct appropriate diagnostic tests and therapeutic interventions to prevent complications and preserve visual integrity in affected individuals.
Active trachoma: This manifests as mixed follicular or papillary conjunctivitis, often associated with mucopurulent discharge. Active trachoma commonly presents with superior epithelial keratitis is commonly seen. Corneal vascularization may lead to the development of pannus.[48][49]
Cicatricial trachoma: This typically presents with stellate or linear conjunctival scars or broad confluent scars (known as Arlt line) in advanced stages. Although the entire conjunctiva is involved, the effects are more prominent on the upper tarsal plate. As follicles in this region resolve, a row of shallow depressions called Herbert pits [50] might be formed in the superior limbus. Trichiasis, distichiasis, corneal vascularization, and entropion can also manifest, often accompanied by severe corneal opacification. Destruction of goblet cells and the ductules of the lacrimal glands eventually leads to dry eyes.[10][51]
Evaluation
The diagnosis of trachoma primarily depends on the patient's history and clinical signs observed during a slit-lamp examination. Although several diagnostic tests have been developed to detect the organism, a universally recognized gold standard investigation does not exist.[52][53] Some of the tests currently used are listed below.
Laboratory Examinations
- Giemsa staining of smears of conjunctival cells to demonstrate the chlamydial inclusion body.
- Cell cultures and microscopy.
- Microbiological testing: This testing method often involves polymerase chain reaction and nucleic acid amplification tests, which are the 2 common molecular techniques used to confirm an active C trachomatis infection in laboratory settings. Conjunctival swabs or scrapings from affected individuals are collected and examined for the presence of C trachomatis DNA. While these methods are valuable for research purposes, they are often considered expensive and complex for routine clinical use.
- Serological testing: This testing method involves detecting antibodies against C trachomatis in serum samples using enzyme-linked immunosorbent assays (ELISAs) or immunofluorescence assays. However, serological testing is primarily utilized in epidemiological research rather than for clinical diagnosis.
Clinical Evaluation
- Trachoma severity grading: WHO has devised a streamlined grading system based on clinical indicators observed during the inspection to categorize the severity of trachoma. This system includes 5 categories—trachomatous trichiasis (TT), corneal opacity (CO), trachomatous inflammation follicular (TF), trachomatous inflammation intense (TI), and trachomatous scarring (TS).[54]
- Trichiasis assessment: This evaluation involves a direct flashlight examination, commonly utilized to identify ingrown eyelashes touching the cornea, which helps determine the presence and severity of trichiasis or eyelash misalignment. During this examination, the number and position of trichiatic eyelashes are recorded to assist in surgical planning.[47]
Radiography and Imaging Techniques
- Radiographic imaging: Radiographic imaging techniques, such as optical coherence tomography or ultrasonography, can be employed to assess structural abnormalities in the eye, particularly in cases of corneal opacity or scarring.
- Extra diagnostic testing: Conjunctival photography and mobile health technology serve as supplementary tools used in certain situations to record clinical observations, monitor and track the course of an illness, and assess treatment effectiveness. Modern techniques helpful for trachoma diagnosis include photography,[55] artificial machine learning approaches,[56] and automated deep learning methods.[57]
Treatment / Management
The SAFE strategy (surgery, antibiotics, facial cleanliness, and environmental improvement) recommended by WHO includes surgery for trichiasis, antibiotics, facial hygiene, and environmental improvement measures.[58]
- Antibiotics should be administered to the patient and all the family members.[59]
- Azithromycin (20 mg/kg up to 1 g), as a single dose, stands out as the preferred antibiotic or treatment of choice, given its effectiveness and convenient dosing regimen, particularly when taken orally either as a single dose or as part of a mass drug administration approach.
- Erythromycin (500 mg twice daily for 14 days) or doxycycline (100 mg twice daily for 10 days) may be considered, although caution is warranted with tetracyclines in pregnancy, breastfeeding, and among children.
- Tetracycline ointment (1%) may be used topically. However, it is less effective than oral treatment.
- Facial cleanliness is important.[60]
- Environmental improvement includes proper sanitation, access to clean drinking water, control of flies, and other relevant measures.[61] (B3)
- Surgical intervention may be necessary to address conditions such as entropion and trichiasis, ensuring functional and complete lid closure (see Image. Surgical Repair of Trachomatous Upper Eyelid Entropion).[62] (B2)
Management of Trichiasis and Cicatricial Entropion
Trachoma is the most common infectious cause of blindness globally, primarily due to conjunctival scarring leading to trichiasis and entropion, ultimately resulting in corneal scarring and eventual blindness. Therefore, effective management of trichiasis and cicatricial entropion in trachoma is imperative to prevent visual disability.[63][64]
Treatment of lashes: A movement to teach simple procedures to ancillary healthcare team members is necessary in areas where this disease is endemic. This will enable early intervention to prevent corneal injury and scarring.[65]
- Simple epilation
- Destruction of eyelash follicles
- Radiofrequency ablation of follicles
- Cryotherapy to lash roots
- Electrocautery
- Laser (argon or other types) treatment of lash roots
- Irradiation (infrequently used now)
- Surgical excision of roots of eyelashes
Surgical repair of trichiasis and entropion: The management of trichiasis and entropion in trachoma involves a range of surgical techniques to correct eyelid abnormalities and prevent corneal damage, as listed below.[66][67](A1)
- Tarsal rotation with bilamellar tarsal rotation or anterior lamellar tarsal rotation
- Tarsal repositioning with tarsal advancement with or without tarsal rotation
- Posterior lamellar lengthening with the advancement of the posterior lamella with or without an interpositional mucous membrane or tarsal graft
- Surgery to the anterior lamellar and eyelid margin
- Anterior lamellar repositioning
- Eyelid margin split and eversion
- Anterior tarsal wedge resection (or grooving) and eversion
- Tarsectomy
Differential Diagnosis
Distinguishing trachoma from other ocular disorders can be challenging due to overlapping clinical features. Therefore, it is crucial to carefully evaluate differential diagnoses to ensure appropriate management and avoid unnecessary treatment.[68]
- Allergic conjunctivitis: The symptoms of allergic conjunctivitis can mimic the clinical signs of trachoma, including redness, itching, tearing, and swelling of the eyelids. Allergic conjunctivitis is usually bilateral and is often associated with prior exposure to allergens such as dust, pollen, or pet dander.
- Bacterial conjunctivitis: Acute bacterial conjunctivitis and trachoma share similar clinical manifestations, such as crusting on the eyelids, discharge, and redness. Bacterial conjunctivitis frequently manifests acutely, with symptoms appearing rapidly and resolving spontaneously. Trachoma, conversely, is characterized by recurrent infections and persistent inflammation typify trachoma (see Image. Bacterial Conjunctivitis).
- Viral conjunctivitis: Adenovirus or herpes simplex virus can induce viral conjunctivitis, exhibiting symptoms similar to trachoma, including photophobia, tearing, and redness. Nonetheless, systemic symptoms, such as fever and malaise, are commonly linked to viral conjunctivitis, which may aid in distinguishing it from trachoma.
- Dry eye syndrome: This condition shares symptoms with trachoma, including redness, ocular discomfort, and a sensation of foreign body presence. However, the hallmark of dry eye syndrome is inadequate tear production or instability of the tear film, leading to dryness and discomfort on the ocular surface.
- Pterygium and pinguecula: Pterygium and pinguecula are benign growths on the conjunctiva that resemble trachoma and can cause redness and irritation. These lesions are usually unilateral and situated next to the limbus, differentiating them from the diffuse conjunctival inflammation in trachoma.
- Giant papillary conjunctivitis: This condition is an inflammatory conjunctivitis characterized by the production of giant papillae and is frequently linked to contact lens wear or ocular prostheses. Although it shares symptoms with trachoma, such as redness and itching, it typically presents bilaterally and has a history of ocular surface irritation.
- Atopic keratoconjunctivitis: This is a persistent inflammatory condition that affects the cornea and conjunctiva and is often linked to atopic dermatitis. Individuals suffering from atopic keratoconjunctivitis may exhibit signs of inflammation of the conjunctiva, including redness, itching, and photophobia, which can resemble those of trachoma. However, atopic keratoconjunctivitis typically presents bilaterally and can be linked to additional systemic atopic symptoms.
- Less common ocular conditions that can exhibit similar signs and symptoms to trachoma include chronic follicular conjunctivitis, Parinaud oculoglandular conjunctivitis, silent dacryocystitis, issues related to contact lens use, and various causes of entropion and trichiasis.
Staging
WHO recommends a simplified grading system for trachoma.[69]
- Trachomatous inflammation, follicular (TF): This is characterized by the presence of five or more lymphoid follicles, each at least 0.5 mm in diameter, in the central region of the upper tarsal conjunctiva.
- Trachomatous inflammation, intense (TI): This manifests as significant inflammatory alterations in the conjunctiva, including pronounced thickening throughout the entire tarsal conjunctiva or marked thickening that obscures more than half of the typical deep tarsal vessels.
- Trachomatous scarring (TS): This is characterized by scarring of the tarsal conjunctiva, which presents as fine, white, horizontal lines parallel to the lid edge or linear lines. This scarring can lead to trichiasis (misaligned eyelashes) and deformities of the conjunctival surface, potentially causing corneal transparency issues.
- Trachomatous trichiasis (TT): This is defined as the presence of at least one eyelash touching the globe or evidence of recently removed inverted eyelashes. TT is associated with recurrent episodes of infection, inflammation, and scarring, leading to potential complications such as corneal abrasions and eyelid abnormalities.
- Corneal opacity (CO): This represents the most advanced stage of trachoma and is characterized by corneal opacification. If left untreated, this condition can lead to blindness and vision impairment.
Prognosis
The prognosis of trachoma is influenced by various factors, including disease stages, comorbidities such as trichiasis and corneal opacities, access to healthcare, and the implementation of therapy and prevention strategies. International efforts, such as adopting the SAFE approach, to contain and eradicate the disease have contributed to recent improvements in the prognosis of trachoma.
Several studies have shown significant reductions in the prevalence of active disease as a result of practicing this strategy.[70][71]
Early-stage trachoma: With prompt and adequate therapy, the prognosis is generally favorable for trachoma patients in their early stages (TF and TI). Antibiotics such as azithromycin and topical tetracycline effectively eliminate C trachomatis infections, reducing the risk of disease progression. Health education initiatives promoting facial cleanliness and environmental modifications are crucial in curtailing disease transmission and preventing reinfection within communities.
Advanced-stage trachoma: In advanced-stage trachoma with scarring (TS), the prognosis may worsen if complications like trichiasis and corneal opacities arise. Untreated trichiasis, characterized by misaligned eyelashes, can lead to corneal abrasions, ulcers, and blindness. However, surgical correction techniques such as posterior lamellar tarsal rotation or bilamellar tarsal rotation can significantly improve outcomes and prevent blindness.
Issues and the extended prognosis: Long-term prognosis in trachoma can be significantly influenced by complications like corneal opacities, neovascularization, and irreversible vision loss. If left untreated, corneal opacity and scarring resulting from recurring infections and persistent inflammation can cause blindness or visual impairment. Nonetheless, in extreme circumstances, some degree of vision restoration might be achievable with the appropriate medical and surgical procedures, including corneal transplantation.
Public health interventions and international initiatives: Efforts to manage and eradicate trachoma globally have led to a notable improvement in the disease's prognosis. Initiatives such as the International Trachoma Initiative (ITI) [72] and the WHO Alliance for the Global Elimination of Trachoma by 2020 have contributed to significant reductions in trachoma prevalence and blindness worldwide.[73][74] Through mass drug administration campaigns, surgical outreach initiatives, and community-based treatments, patient outcomes have been enhanced, and access to care has improved.[75]
Although trachoma remains a significant public health concern, particularly in resource-limited regions, advancements in diagnosis, prevention, and treatment have led to improved prognoses and outcomes for affected individuals. However, achieving global trachoma elimination and preventing unnecessary blindness requires sustained funding for trachoma control programs, research endeavors, and advocacy initiatives.[76]
Complications
Undiagnosed or improperly managed trachoma can cause several issues that can eventually lead to blindness and permanent vision impairment.[77] Recurring infections, persistent inflammation, and disease-related tissue scarring frequently bring on these adverse effects. Some of the main complications associated with trachoma are listed below.
- Trichiasis: Trichiasis refers to the misalignment of lashes, leading to repetitive abrasion of the corneal surface with each blink. Over time, this irritation can cause corneal abrasions, ulcerations, and scarring from misdirected eyelashes that irritate and rub the cornea. Without proper treatment, trichiasis can progress to corneal opacities and eventual blindness.
- Entropion: Entropion occurs when the eyelid turns inward, causing the lashes to scrape on the eye's surface, resulting in discomfort, corneal abrasions, and potential blindness if left untreated. Entropion is a consequence of advanced trachoma in which the eyelids compress inward due to scarring and recurrent infections.
- Distichiasis: This condition occurs when an additional row of lashes grows along the eyelid's edge, pointing toward the direction of the eye. These unusual eyelashes can cause pain, redness, and even corneal injury by irritating the cornea. Severe trachoma-related eyelid deformities and scarring can lead to this condition.
- Dry eye syndrome: This syndrome can be triggered by the detrimental impact of trachoma on the cornea and conjunctiva, diminishing tear production and compromising tear film integrity. Symptoms include redness, burning, itching, and impaired vision. Chronic dryness also elevates the risk of eye infections and other complications.
- Superadded bacterial infection: The chronic inflammation and scarring associated with trachoma can compromise the eye's immune system, heightening susceptibility to secondary bacterial infections. If left untreated, these infections can exacerbate trachoma symptoms, leading to conditions like conjunctivitis, corneal ulcers, and potentially blindness. Effective management often necessitates antibiotic therapy.
- Corneal opacities: Usually a consequence of trachoma, corneal opacities result from prolonged inflammation and scarring of the cornea. These opacities may cause reduced visual acuity and possibly irreversible vision loss by interfering with light's ability to enter the eye. Dense corneal opacities can obstruct the pupil and cause central vision impairments in severe situations.
- Corneal neovascularization: Corneal neovascularization, a complication of trachoma, involves the chronic inflammation and vascularization of the cornea. This abnormal blood vessel growth can disrupt the eye's natural optical properties, leading to compromised corneal transparency and potentially resulting in visual impairment.
- Conjunctival scarring: Recurrent episodes of inflammation in trachoma may cause conjunctival scarring, characterized by fibrosis and alteration of the architecture and texture of the surrounding tissue. This scarring on the conjunctiva may worsen ocular surface dryness, destabilize the tear film, and increase the risk of corneal problems and subsequent infections.
- Blindness: Trachoma, if left untreated or inadequately managed, can lead to irreversible blindness, particularly in cases of severe trichiasis, corneal opacities, or other issues impacting visual function. Blindness caused by trachoma not only affects individuals but also has profound socioeconomic repercussions on their communities, significantly impacting their quality of life.
Deterrence and Patient Education
Patient education should emphasize the importance of avoiding overcrowding and maintaining good hygiene practices. Minimizing hand-eye contact and refraining from frequently touching the eyes are essential. Encouraging good hygiene practices, such as regular handwashing, is crucial. Education should stress the importance of maintaining facial hygiene by washing the face frequently with soap and water to prevent the spread of C trachomatis–containing ocular secretions. People in endemic areas should be advised to dry their faces with clean towels or tissues and avoid sharing personal items such as washcloths and towels.
Emphasizing frequent handwashing is essential to prevent the transfer of bacteria from feces to the mouth, particularly before handling food and after using the restroom. Improvements to water, sanitation, and hygiene (WASH) infrastructure are necessary to reduce environmental contamination and the risk of trachoma transmission. This includes ensuring access to clean water sources, sanitation facilities, and effective waste management systems. Upgrading sanitation infrastructure and promoting proper waste disposal techniques through community-led environmental sanitation projects are critical steps in this effort.
Residents of high-risk regions should receive education about the warning signs and symptoms of trachoma, such as redness, irritation, discharge, and blurred vision, to promote early detection and treatment-seeking behavior. Patients should understand the importance of seeking treatment for eye infections and ocular diseases from qualified medical professionals, emphasizing the effectiveness of available medications like antibiotics. Community-based health education programs involving the community in prevention and control initiatives can aid trachoma prevention and patient treatment. Culturally relevant resources and communication strategies must be used for effective outreach.
Infected individuals should immediately be quarantined from the rest of their family members, friends, and associates to prevent further transmission. Upon diagnosis, patients must receive comprehensive education on the disease, its modes of transmission, and preventive measures. They should also be informed about potential complications resulting from noncompliance or treatment failure.
Fundamental initiatives are needed to enable people and communities to adopt proactive measures toward trachoma prevention and control by implementing comprehensive deterrence and patient education programs guided by national and international recommendations. These initiatives depend on eliminating trachoma worldwide and improving the health and well-being of affected individuals.
Pearls and Other Issues
Trachoma, the leading infectious cause of blindness globally, predominantly affects populations in underdeveloped areas with limited access to healthcare and sanitary facilities. C trachomatis bacterium, which causes the disease, is spread via ocular and nasal secretions, contaminated hands, and fomites. The disease initially presents as focal conjunctivitis (TF) and severe inflammation (TI). Trachoma-induced blindness ranks as the primary infectious cause of blindness, with scarring (TS) and potentially blinding consequences, such as trichiasis and corneal opacities (TT), following. Trachoma control relies on the SAFE strategy, which entails mass pharmacological administration, surgical trichiasis correction, and hygiene promotion.
Patients diagnosed with trachoma, particularly those with corneal opacities or trichiasis, may necessitate referral to ophthalmologists or other specialized eye care providers for further evaluation and treatment. Antibiotic therapy may be required for individuals with active trachoma to eliminate the infection and halt disease progression, while surgical intervention may be necessary for those experiencing complications to preserve their vision.
In endemic regions, efforts to manage trachoma may face challenges due to limited resources, cultural barriers, and inadequate healthcare access. Inadequate surveillance and monitoring systems and delays in implementing control measures can lead to underreporting trachoma cases. Additionally, irregular or incomplete adherence to treatment plans and antibiotic resistance may compromise the effectiveness of mass drug administration programs.
Blindness resulting from trachoma is preventable through measures such as improved hygiene, sanitation, and environmental modifications to reduce bacterial transmission. Health education and community engagement are crucial in raising awareness, early detection, and promoting behavioral changes. Comprehensive trachoma control initiatives, supported by global partnerships, are crucial for sustained eradication of the disease. Clinicians and medical staff in endemic regions should receive training in basic techniques such as epilation and surgical procedures to address trachoma effectively.
Enhancing Healthcare Team Outcomes
Trachoma is a prevalent infection that often presents to primary care or emergency department providers. These providers should consult ophthalmologists before initiating treatment to ensure timely and appropriate care and minimize morbidity. Effective management of trachoma involves an interprofessional healthcare team comprising physicians, nurses, pharmacists, laboratory staff, and transfusion specialists. This collaborative approach aims to deliver patient-centered care, improve outcomes, ensure safety, and optimize team performance.
Collaboration among healthcare professionals is crucial for optimal patient outcomes in trachoma management. Ophthalmologists, optometrists, dermatologists, nurses, and pharmacists must collaborate to comprehensively address the disease and its potential complications. Continuous follow-up, monitoring symptoms, and ensuring normal visual acuity post-treatment are essential, with surgeons involved as needed for surgical interventions to prevent complications. Effective interprofessional communication is fundamental in addressing the core issues of trachoma management.
An interprofessional team approach and effective communication among healthcare providers is essential in trachoma management. Prompt recognition of symptoms by physicians and nurses, including eyelid and eye irritation, redness, itching, swelling, discharge, eye pain, and photophobia, is crucial. Laboratory staff should ensure accurate cross-matching and compatibility checks. Effective communication among team members ensures rapid diagnosis and treatment decisions by minimizing errors and providing a coordinated response. Clinicians make treatment decisions and prescribe appropriate therapy. Nursing staff can support patient education and assess therapeutic effectiveness. Pharmacists verify dosing and reconcile medications to prevent drug-drug interactions. Any concerns from nursing or pharmacy should be promptly communicated to the treating clinicians. This interprofessional, collaborative approach optimizes trachoma management, resulting in improved patient outcomes.
Continuous education and training are essential for keeping the healthcare team informed about best practices in trachoma management. Regular professional development enables healthcare practitioners to diagnose trachoma and promptly respond effectively to appropriate treatment options. A patient-centered approach prioritizes the patient's well-being and preferences in all decisions. An interprofessional healthcare team is crucial in managing trachoma infection, reducing the risk of transmission, providing comprehensive care, minimizing complications, and ensuring patient safety and quality of care.
Media
(Click Image to Enlarge)
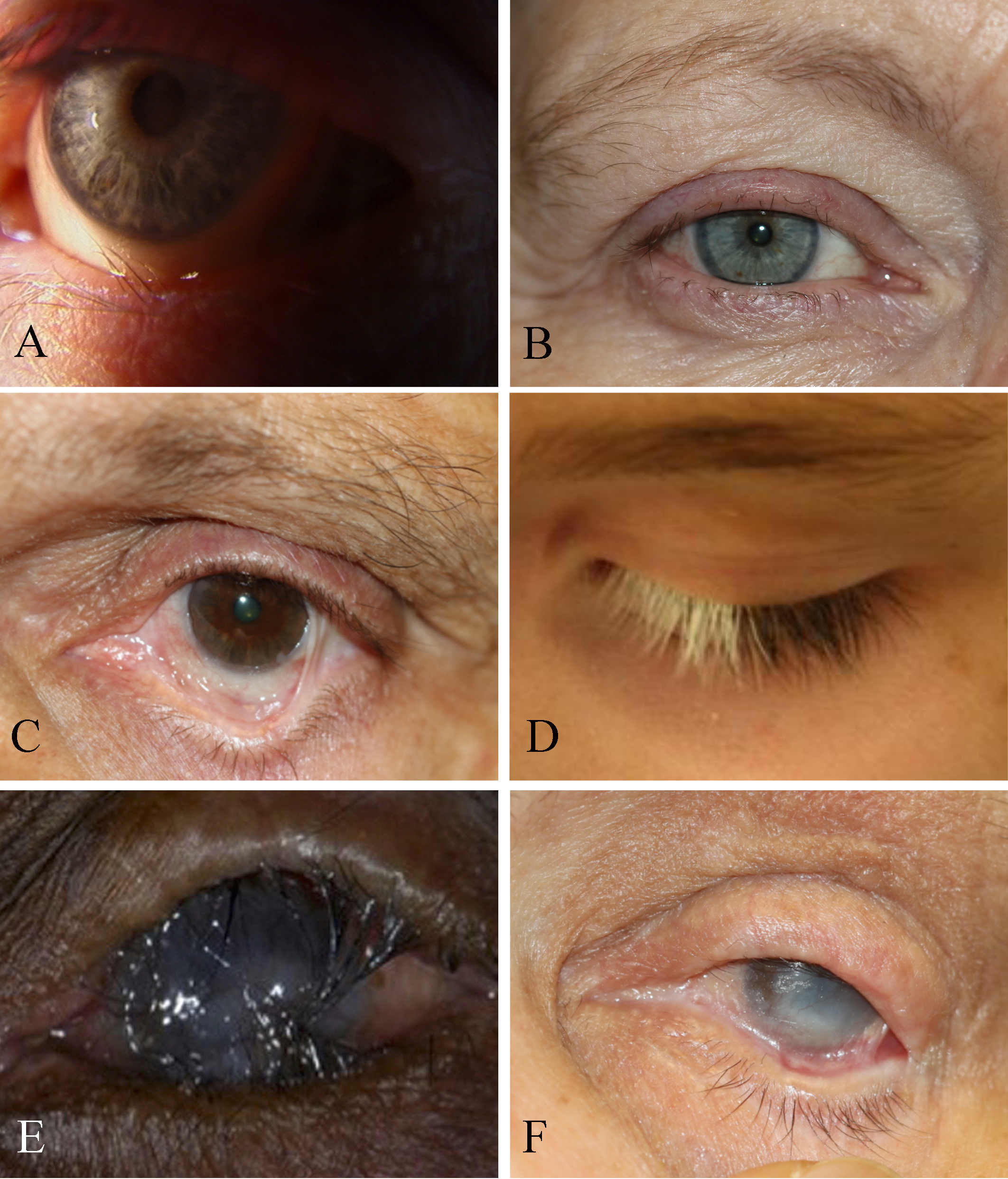
Eye Disorders and Trachoma-Associated Symptoms, Trichiasis. The eyelid itself is not turning in, but the lashes are pointing inward (A). Madarosis. Short stubby lashes of different sizes indicate trichotillomania (B). Symblepharon with secondary trichiasis, fornix shortening, and cicatricial entropion (C). Poliosis (D). Trachoma with corneal opacification (E). Pemphigoid disease with cicatricial entropion, trichiasis, ankyloblepharon, corneal scarring, and dry eyes (F).
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Bacterial Conjunctivitis
Contributed by O Chaigasame, MD
(Click Image to Enlarge)

Surgical Repair of Trachomatous Upper Eyelid Entropion. The images depict surgical correction of trachomatous upper eyelid entropion using Trabut-type eversion and mucous membrane graft. Preoperative appearance showing posterior lamellar shortening, scarred conjunctiva, and tarsal plate (A). Postoperative appearance following Trabut procedure and mucous membrane grafting (B). Appearance after a 2-year follow-up demonstrates successful correction of the upper eyelid entropion, resulting in a quiet, comfortable eye with a clear cornea (C).
Contributed by BCK Patel, MD, FRCS
References
Pintea-Trifu ML, Bâlici Ş, Siserman CV, Vică ML, Matei HV. Chlamydia trachomatis and the HLA involvement in the development of infection and disease: a narrative review. Medicine and pharmacy reports. 2023 Oct:96(4):335-345. doi: 10.15386/mpr-2593. Epub 2023 Oct 26 [PubMed PMID: 37970191]
Level 3 (low-level) evidenceHarding-Esch EM, Holland MJ, Schémann JF, Sissoko M, Sarr B, Butcher RMR, Molina-Gonzalez S, Andreasen AA, Mabey DCW, Bailey RL. Facial cleanliness indicators by time of day: results of a cross-sectional trachoma prevalence survey in Senegal. Parasites & vectors. 2020 Nov 18:13(1):556. doi: 10.1186/s13071-020-04410-w. Epub 2020 Nov 18 [PubMed PMID: 33203456]
Level 2 (mid-level) evidenceFlaxman SR, Bourne RRA, Resnikoff S, Ackland P, Braithwaite T, Cicinelli MV, Das A, Jonas JB, Keeffe J, Kempen JH, Leasher J, Limburg H, Naidoo K, Pesudovs K, Silvester A, Stevens GA, Tahhan N, Wong TY, Taylor HR, Vision Loss Expert Group of the Global Burden of Disease Study. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. The Lancet. Global health. 2017 Dec:5(12):e1221-e1234. doi: 10.1016/S2214-109X(17)30393-5. Epub 2017 Oct 11 [PubMed PMID: 29032195]
Level 1 (high-level) evidenceWang EY, Kong X, Wolle M, Gasquet N, Ssekasanvu J, Mariotti SP, Bourne R, Taylor H, Resnikoff S, West S. Global Trends in Blindness and Vision Impairment Resulting from Corneal Opacity 1984-2020: A Meta-analysis. Ophthalmology. 2023 Aug:130(8):863-871. doi: 10.1016/j.ophtha.2023.03.012. Epub 2023 Mar 22 [PubMed PMID: 36963570]
Level 1 (high-level) evidenceQuesada-Cubo V, Damián-González DC, Prado-Velasco FG, Fernández-Santos NA, Sánchez-Tejeda G, Correa-Morales F, Domínguez-Zárate H, García-Orozco A, Saboyá-Díaz MI, Sánchez-Martín MJ. The elimination of trachoma as a public health problem in Mexico: From national health priority to national success story. PLoS neglected tropical diseases. 2022 Aug:16(8):e0010660. doi: 10.1371/journal.pntd.0010660. Epub 2022 Aug 29 [PubMed PMID: 36037211]
Hadfield J, Harris SR, Seth-Smith HMB, Parmar S, Andersson P, Giffard PM, Schachter J, Moncada J, Ellison L, Vaulet MLG, Fermepin MR, Radebe F, Mendoza S, Ouburg S, Morré SA, Sachse K, Puolakkainen M, Korhonen SJ, Sonnex C, Wiggins R, Jalal H, Brunelli T, Casprini P, Pitt R, Ison C, Savicheva A, Shipitsyna E, Hadad R, Kari L, Burton MJ, Mabey D, Solomon AW, Lewis D, Marsh P, Unemo M, Clarke IN, Parkhill J, Thomson NR. Comprehensive global genome dynamics of Chlamydia trachomatis show ancient diversification followed by contemporary mixing and recent lineage expansion. Genome research. 2017 Jul:27(7):1220-1229. doi: 10.1101/gr.212647.116. Epub 2017 Jun 6 [PubMed PMID: 28588068]
Kitu M, Mihretie K, Abuhay T. Case-control study of determinants of corrective upper eyelid surgery refusals among trachomatous trichiasis patients in Ethiopia. Eastern Mediterranean health journal = La revue de sante de la Mediterranee orientale = al-Majallah al-sihhiyah li-sharq al-mutawassit. 2023 Nov 30:26(11):903-911. doi: 10.26719/emhj.23.085. Epub 2023 Nov 30 [PubMed PMID: 38279886]
Level 2 (mid-level) evidenceKreis AJ, Nouhoum G. Comment on: Recurrent upper eyelid trachomatous entropion repair: long-term efficacy of a five-step approach. Eye (London, England). 2022 Dec:36(12):2364. doi: 10.1038/s41433-022-01974-y. Epub 2022 May 7 [PubMed PMID: 35525859]
Level 3 (low-level) evidenceCochrane GM, Mangot M, Houinei W, Susapu M, Cama A, Le Mesurier R, Webster S, Hillgrove T, Barton J, Butcher R, Harding-Esch EM, Mabey D, Bakhtiari A, Müller A, Yajima A, Solomon AW, Kaldor J, Koim SP, Ko R, Garap J. Corneal pannus, Herbert's pits and conjunctival inflammation in older children in Papua New Guinea. Ophthalmic epidemiology. 2024 Feb 8:():1-8. doi: 10.1080/09286586.2023.2273507. Epub 2024 Feb 8 [PubMed PMID: 38329811]
Solomon AW, Burton MJ, Gower EW, Harding-Esch EM, Oldenburg CE, Taylor HR, Traoré L. Trachoma. Nature reviews. Disease primers. 2022 May 26:8(1):32. doi: 10.1038/s41572-022-00359-5. Epub 2022 May 26 [PubMed PMID: 35618795]
Genet A, Dagnew Z, Melkie G, Keleb A, Motbainor A, Mebrat A, Leshargie CT. Prevalence of active trachoma and its associated factors among 1-9 years of age children from model and non-model kebeles in Dangila district, northwest Ethiopia. PloS one. 2022:17(6):e0268441. doi: 10.1371/journal.pone.0268441. Epub 2022 Jun 15 [PubMed PMID: 35704657]
Robinson A, Gomes LRO, Abdurahman OS, Alemayehu W, Shuka G, Melese E, Guye M, Legesse D, Elias E, Temam K, Koro KH, Adugna D, Seife F, Aga MA, Sarah V, Lambert SM, Walker SL, Habtamu E, Solomon AW, Last A, Macleod D, Burton MJ, Logan JG. Evaluation of the efficacy of insecticide-treated scarves to protect children from the trachoma vector Musca sorbens (Diptera: Muscidae): A phase II randomised controlled trial in Oromia, Ethiopia. EClinicalMedicine. 2022 Jul:49():101487. doi: 10.1016/j.eclinm.2022.101487. Epub 2022 Jun 8 [PubMed PMID: 35747196]
Level 1 (high-level) evidenceLast A, Versteeg B, Shafi Abdurahman O, Robinson A, Dumessa G, Abraham Aga M, Shumi Bejiga G, Negussu N, Greenland K, Czerniewska A, Thomson N, Cairncross S, Sarah V, Macleod D, Solomon AW, Logan J, Burton MJ. Detecting extra-ocular Chlamydia trachomatis in a trachoma-endemic community in Ethiopia: Identifying potential routes of transmission. PLoS neglected tropical diseases. 2020 Mar:14(3):e0008120. doi: 10.1371/journal.pntd.0008120. Epub 2020 Mar 4 [PubMed PMID: 32130213]
Jones BR. The prevention of blindness from trachoma. Transactions of the ophthalmological societies of the United Kingdom. 1975 Apr:95(1):16-33 [PubMed PMID: 775692]
Level 3 (low-level) evidenceMarques AP, Ramke J, Cairns J, Butt T, Zhang JH, Jones I, Jovic M, Nandakumar A, Faal H, Taylor H, Bastawrous A, Braithwaite T, Resnikoff S, Khaw PT, Bourne R, Gordon I, Frick K, Burton MJ. The economics of vision impairment and its leading causes: A systematic review. EClinicalMedicine. 2022 Apr:46():101354. doi: 10.1016/j.eclinm.2022.101354. Epub 2022 Mar 22 [PubMed PMID: 35340626]
Level 1 (high-level) evidenceDerrick T, Roberts Ch, Last AR, Burr SE, Holland MJ. Trachoma and Ocular Chlamydial Infection in the Era of Genomics. Mediators of inflammation. 2015:2015():791847. doi: 10.1155/2015/791847. Epub 2015 Sep 3 [PubMed PMID: 26424969]
Gallenga CE, Maritati M, Del Boccio M, D'Aloisio R, Conti P, Mura M, Contini C, Gallenga PE. Why the SAFE-S Strategy for Trachoma? Are Musca sorbens or Scatophaga stercoraria Really the Culprit?-A Brief Historical Review from an Italian Point of View. Pathogens (Basel, Switzerland). 2023 Dec 4:12(12):. doi: 10.3390/pathogens12121419. Epub 2023 Dec 4 [PubMed PMID: 38133302]
Dzakah EE, Huang L, Xue Y, Wei S, Wang X, Chen H, Shui J, Kyei F, Rashid F, Zheng H, Yang B, Tang S. Host cell response and distinct gene expression profiles at different stages of Chlamydia trachomatis infection reveals stage-specific biomarkers of infection. BMC microbiology. 2021 Jan 4:21(1):3. doi: 10.1186/s12866-020-02061-6. Epub 2021 Jan 4 [PubMed PMID: 33397284]
Lynch KD, Morotti W, Brian G, Ketchup L, Kingston K, Starr M, Ware RS, Everill B, Asgar N, O'Keefe A, Whop LJ, Kaldor JM, Lambert SB. Clinical signs of trachoma and laboratory evidence of ocular Chlamydia trachomatis infection in a remote Queensland community: a serial cross-sectional study. The Medical journal of Australia. 2022 Nov 21:217(10):538-543. doi: 10.5694/mja2.51735. Epub 2022 Sep 30 [PubMed PMID: 36180097]
Level 2 (mid-level) evidenceYang C, Kari L, Lei L, Carlson JH, Ma L, Couch CE, Whitmire WM, Bock K, Moore I, Bonner C, McClarty G, Caldwell HD. Chlamydia trachomatis Plasmid Gene Protein 3 Is Essential for the Establishment of Persistent Infection and Associated Immunopathology. mBio. 2020 Aug 18:11(4):. doi: 10.1128/mBio.01902-20. Epub 2020 Aug 18 [PubMed PMID: 32817110]
Resnikoff S, Pascolini D, Etya'ale D, Kocur I, Pararajasegaram R, Pokharel GP, Mariotti SP. Global data on visual impairment in the year 2002. Bulletin of the World Health Organization. 2004 Nov:82(11):844-51 [PubMed PMID: 15640920]
Thylefors B, Négrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness. Bulletin of the World Health Organization. 1995:73(1):115-21 [PubMed PMID: 7704921]
Polack S, Brooker S, Kuper H, Mariotti S, Mabey D, Foster A. Mapping the global distribution of trachoma. Bulletin of the World Health Organization. 2005 Dec:83(12):913-9 [PubMed PMID: 16462983]
. Trachoma. Nature reviews. Disease primers. 2022 May 26:8(1):33. doi: 10.1038/s41572-022-00369-3. Epub 2022 May 26 [PubMed PMID: 35618865]
Al-Khatib T, Bella AL, Saboyá-Díaz MI, Solomon AW. Trachoma: The Last Decade? Ophthalmic epidemiology. 2023 Dec:30(6):541-543. doi: 10.1080/09286586.2023.2270045. Epub 2023 Dec 12 [PubMed PMID: 38085790]
Ono K, Umeya R. Longitudinal Analysis of Eye Health Disparities Due to Trachoma Using Country-Level Data from the Global Burden of Disease Study 2019. Ophthalmic epidemiology. 2023 Mar 7:():1-7. doi: 10.1080/09286586.2023.2188561. Epub 2023 Mar 7 [PubMed PMID: 36882966]
Impouma B, Kalu AA, Makubalo L, Gasasira A, Cabore J, Moeti M. Responding to Africa's burden of disease: accelerating progress. Epidemiology and infection. 2023 Jun 20:151():e114. doi: 10.1017/S0950268823000997. Epub 2023 Jun 20 [PubMed PMID: 37337304]
Ageed A, Khan M. Eliminating Trachoma in Africa: The Importance of Environmental Interventions. Cureus. 2024 Jan:16(1):e52358. doi: 10.7759/cureus.52358. Epub 2024 Jan 16 [PubMed PMID: 38234389]
Altaseb T, Lingerew M, Adane M. Prevalence of trachomatous inflammation-follicular and associated factors among children aged 1-9 years in northeastern Ethiopia. BMC pediatrics. 2024 Feb 19:24(1):128. doi: 10.1186/s12887-024-04587-4. Epub 2024 Feb 19 [PubMed PMID: 38373921]
Cromwell EA, Courtright P, King JD, Rotondo LA, Ngondi J, Emerson PM. The excess burden of trachomatous trichiasis in women: a systematic review and meta-analysis. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2009 Oct:103(10):985-92. doi: 10.1016/j.trstmh.2009.03.012. Epub 2009 Apr 10 [PubMed PMID: 19362326]
Level 1 (high-level) evidenceHarding-Esch EM, Burgert-Brucker CR, Jimenez C, Bakhtiari A, Willis R, Bejiga MD, Mpyet C, Ngondi J, Boyd S, Abdala M, Abdou A, Adamu Y, Alemayehu A, Alemayehu W, Al-Khatib T, Apadinuwe SC, Awaca N, Awoussi MS, Baayendag G, Badiane MD, Bailey RL, Batcho W, Bay Z, Bella A, Beido N, Bol YY, Bougouma C, Brady CJ, Bucumi V, Butcher R, Cakacaka R, Cama A, Camara M, Cassama E, Chaora SG, Chebbi AC, Chisambi AB, Chu B, Conteh A, Coulibaly SM, Courtright P, Dalmar A, Dat TM, Davids T, Djaker MEA, de Fátima Costa Lopes M, Dézoumbé D, Dodson S, Downs P, Eckman S, Elshafie BE, Elmezoghi M, Elvis AA, Emerson P, Epée EE, Faktaufon D, Fall M, Fassinou A, Fleming F, Flueckiger R, Gamael KK, Garae M, Garap J, Gass K, Gebru G, Gichangi MM, Giorgi E, Goépogui A, Gómez DVF, Gómez Forero DP, Gower EW, Harte A, Henry R, Honorio-Morales HA, Ilako DR, Issifou AAB, Jones E, Kabona G, Kabore M, Kadri B, Kalua K, Kanyi SK, Kebede S, Kebede F, Keenan JD, Kello AB, Khan AA, Khelifi H, Kilangalanga J, Kim SH, Ko R, Lewallen S, Lietman T, Logora MSY, Lopez YA, MacArthur C, Macleod C, Makangila F, Mariko B, Martin DL, Masika M, Massae P, Massangaie M, Matendechero HS, Mathewos T, McCullagh S, Meite A, Mendes EP, Abdi HM, Miller H, Minnih A, Mishra SK, Molefi T, Mosher A, M'Po N, Mugume F, Mukwiza R, Mwale C, Mwatha S, Mwingira U, Nash SD, Nassa C, Negussu N, Nieba C, Noah Noah JC, Nwosu CO, Olobio N, Opon R, Pavluck A, Phiri I, Rainima-Qaniuci M, Renneker KK, Saboyá-Díaz MI, Sakho F, Sanha S, Sarah V, Sarr B, Szwarcwald CL, Shah Salam A, Sharma S, Seife F, Serrano Chavez GM, Sissoko M, Sitoe HM, Sokana O, Tadesse F, Taleo F, Talero SL, Tarfani Y, Tefera A, Tekeraoi R, Tesfazion A, Traina A, Traoré L, Trujillo-Trujillo J, Tukahebwa EM, Vashist P, Wanyama EB, Warusavithana SDP, Watitu TK, West S, Win Y, Woods G, Yajima A, Yaya G, Zecarias A, Zewengiel S, Zoumanigui A, Hooper PJ, Millar T, Rotondo L, Solomon AW. Tropical Data: Approach and Methodology as Applied to Trachoma Prevalence Surveys. Ophthalmic epidemiology. 2023 Dec:30(6):544-560. doi: 10.1080/09286586.2023.2249546. Epub 2023 Dec 12 [PubMed PMID: 38085791]
Level 3 (low-level) evidenceGetachew D, Woldekidan F, Ayele G, Bekele Y, Sleshi S, Tekalgn E, Worku T, Ayenew M, Bogale B, Asres A. High prevalence of active trachoma and associated factors among school-aged children in Southwest Ethiopia. PLoS neglected tropical diseases. 2023 Dec:17(12):e0011846. doi: 10.1371/journal.pntd.0011846. Epub 2023 Dec 15 [PubMed PMID: 38100523]
Derrick T, Ramadhani AM, Macleod D, Massae P, Mafuru E, Aiweda M, Mbuya K, Makupa W, Mtuy T, Bailey RL, Mabey DCW, Holland MJ, Burton MJ. Immunopathogenesis of Progressive Scarring Trachoma: Results of a 4-Year Longitudinal Study in Tanzanian Children. Infection and immunity. 2020 Mar 23:88(4):. doi: 10.1128/IAI.00629-19. Epub 2020 Mar 23 [PubMed PMID: 31964744]
Tidke SC, Tidake P. A Review of Corneal Blindness: Causes and Management. Cureus. 2022 Oct:14(10):e30097. doi: 10.7759/cureus.30097. Epub 2022 Oct 9 [PubMed PMID: 36381769]
Gupta N, Yadav S, Solomon AW, Jain S, Kashyap S, Vanathi M, Tandon R. Atypical Corneal Phenotype in Patients With Trachoma and Secondary Amyloidosis. Cornea. 2022 May 1:41(5):609-615. doi: 10.1097/ICO.0000000000002791. Epub [PubMed PMID: 34176916]
Jury B, Fleming C, Huston WM, Luu LDW. Molecular pathogenesis of Chlamydia trachomatis. Frontiers in cellular and infection microbiology. 2023:13():1281823. doi: 10.3389/fcimb.2023.1281823. Epub 2023 Oct 18 [PubMed PMID: 37920447]
Mandel C, Yang H, Buchko GW, Abendroth J, Grieshaber N, Chiarelli T, Grieshaber S, Omsland A. Expression and structure of the Chlamydia trachomatis DksA ortholog. Pathogens and disease. 2022 May 23:80(1):. doi: 10.1093/femspd/ftac007. Epub [PubMed PMID: 35388904]
Kechagia JZ, Ezra DG, Burton MJ, Bailly M. Fibroblasts profiling in scarring trachoma identifies IL-6 as a functional component of a fibroblast-macrophage pro-fibrotic and pro-inflammatory feedback loop. Scientific reports. 2016 Jun 20:6():28261. doi: 10.1038/srep28261. Epub 2016 Jun 20 [PubMed PMID: 27321784]
Abu el-Asrar AM, Geboes K, Tabbara KF, al-Kharashi SA, Missotten L, Desmet V. Immunopathogenesis of conjunctival scarring in trachoma. Eye (London, England). 1998:12 ( Pt 3a)():453-60 [PubMed PMID: 9775249]
Abu el-Asrar AM, Geboes K, al-Kharashi SA, Tabbara KF, Missotten L. Collagen content and types in trachomatous conjunctivitis. Eye (London, England). 1998:12 ( Pt 4)():735-9 [PubMed PMID: 9850275]
al-Rajhi AA, Hidayat A, Nasr A, al-Faran M. The histopathology and the mechanism of entropion in patients with trachoma. Ophthalmology. 1993 Sep:100(9):1293-6 [PubMed PMID: 8371914]
Ghaem-Maghami S, Bailey RL, Mabey DC, Hay PE, Mahdi OS, Joof HM, Whittle HC, Ward ME, Lewis DJ. Characterization of B-cell responses to Chlamydia trachomatis antigens in humans with trachoma. Infection and immunity. 1997 Dec:65(12):4958-64 [PubMed PMID: 9393782]
Hu VH, Massae P, Weiss HA, Cree IA, Courtright P, Mabey DC, Bailey RL, Burton MJ. In vivo confocal microscopy of trachoma in relation to normal tarsal conjunctiva. Ophthalmology. 2011 Apr:118(4):747-54. doi: 10.1016/j.ophtha.2010.08.029. Epub 2010 Nov 5 [PubMed PMID: 21055819]
Ramadhani AM, Derrick T, Macleod D, Massae P, Mtuy T, Jeffries D, Roberts CH, Bailey RL, Mabey DCW, Holland MJ, Burton MJ. Immunofibrogenic Gene Expression Patterns in Tanzanian Children with Ocular Chlamydia trachomatis Infection, Active Trachoma and Scarring: Baseline Results of a 4-Year Longitudinal Study. Frontiers in cellular and infection microbiology. 2017:7():406. doi: 10.3389/fcimb.2017.00406. Epub 2017 Sep 15 [PubMed PMID: 28966918]
Lynch KD, Brian G, Ahwang T, Newie T, Newie V, Perrett C, Wharton G, Brown A, Tozer S, Kaldor JM, Whop LJ, Andrews RM, Lambert SB. Discord between presence of follicular conjunctivitis and Chlamydia trachomatis infection in a single Torres Strait Island community: a cross-sectional survey. Australian and New Zealand journal of public health. 2022 Apr:46(2):155-160. doi: 10.1111/1753-6405.13179. Epub 2022 Jan 3 [PubMed PMID: 34978363]
Level 2 (mid-level) evidenceGallini JW, Sata E, Zerihun M, Melak B, Haile M, Zeru T, Gessese D, Ayele Z, Tadesse Z, Callahan EK, Nash SD, Weiss PS. Optimizing cluster survey designs for estimating trachomatous inflammation-follicular within trachoma control programs. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2022 Mar:116():101-107. doi: 10.1016/j.ijid.2021.12.355. Epub 2021 Dec 26 [PubMed PMID: 34965463]
Level 3 (low-level) evidenceDiallo AO, Bayissasse B, Sisay A, Seyum D, Weaver J, Munoz B, Merbs SL, Gower EW. Effectiveness of Trachomatous Trichiasis Case-identification Approaches in Ethiopia. Epidemiology (Cambridge, Mass.). 2023 Nov 1:34(6):909-920. doi: 10.1097/EDE.0000000000001656. Epub 2023 Sep 26 [PubMed PMID: 37757880]
Level 3 (low-level) evidenceBelsti Y, Fekadu SA, Assem AS. Active trachoma prevalence and its associated factors among children aged 1-9 years in rural residents of Lare District, Southwest Ethiopia. International journal of ophthalmology. 2021:14(11):1756-1764. doi: 10.18240/ijo.2021.11.16. Epub 2021 Nov 18 [PubMed PMID: 34804867]
Delelegn D, Tolcha A, Beyene H, Tsegaye B. Status of active trachoma infection among school children who live in villages of open field defecation: a comparative cross-sectional study. BMC public health. 2021 Nov 9:21(1):2051. doi: 10.1186/s12889-021-12106-8. Epub 2021 Nov 9 [PubMed PMID: 34753484]
Level 2 (mid-level) evidenceMustafa O, Daoud YJ. Herbert Pits in Trachoma Infection. Mayo Clinic proceedings. 2020 Jan:95(1):134-135. doi: 10.1016/j.mayocp.2019.10.027. Epub [PubMed PMID: 31902408]
Wang Y, Yuan Y, Pang L, Qiu B, Su D, Guan X, Xiang X, Li J. The upper eyelid levator weakening procedure for the correction of severe cicatricial entropion caused by trachoma. Annals of palliative medicine. 2020 Nov:9(6):4113-4118. doi: 10.21037/apm-20-2067. Epub [PubMed PMID: 33302671]
Level 2 (mid-level) evidenceSchachter J, Moncada J, Dawson CR, Sheppard J, Courtright P, Said ME, Zaki S, Hafez SF, Lorincz A. Nonculture methods for diagnosing chlamydial infection in patients with trachoma: a clue to the pathogenesis of the disease? The Journal of infectious diseases. 1988 Dec:158(6):1347-52 [PubMed PMID: 3058819]
Solomon AW, Peeling RW, Foster A, Mabey DC. Diagnosis and assessment of trachoma. Clinical microbiology reviews. 2004 Oct:17(4):982-1011, table of contents [PubMed PMID: 15489358]
Solomon AW, Kello AB, Bangert M, West SK, Taylor HR, Tekeraoi R, Foster A. The simplified trachoma grading system, amended. Bulletin of the World Health Organization. 2020 Oct 1:98(10):698-705. doi: 10.2471/BLT.19.248708. Epub 2020 Sep 3 [PubMed PMID: 33177759]
Naufal F, West SK, Brady CJ. Utility of photography for trachoma surveys: A systematic review. Survey of ophthalmology. 2022 May-Jun:67(3):842-857. doi: 10.1016/j.survophthal.2021.08.005. Epub 2021 Aug 20 [PubMed PMID: 34425127]
Level 1 (high-level) evidenceSocia D, Brady CJ, West SK, Cockrell RC. Detection of trachoma using machine learning approaches. PLoS neglected tropical diseases. 2022 Dec:16(12):e0010943. doi: 10.1371/journal.pntd.0010943. Epub 2022 Dec 7 [PubMed PMID: 36477293]
Milad D, Antaki F, Robert MC, Duval R. Development and deployment of a smartphone application for diagnosing trachoma: Leveraging code-free deep learning and edge artificial intelligence. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2023 Jul-Sep:37(3):200-206. doi: 10.4103/sjopt.sjopt_106_22. Epub 2023 Feb 16 [PubMed PMID: 38074296]
West SK. Milestones in the fight to eliminate trachoma. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2020 Mar:40(2):66-74. doi: 10.1111/opo.12666. Epub 2020 Feb 3 [PubMed PMID: 32017172]
Sanders AM, Makoy S, Deathe AR, Ohidor S, Jesudason TC, Nute AW, Odongi P, Boniface L, Abuba S, Delahaut AS, Sebit W, Niquette J, Callahan EK, Walker DG, Nash SD. Cost and community acceptability of enhanced antibiotic distribution approaches for trachoma in the Republic of South Sudan: enhancing the A in SAFE (ETAS) study protocol. BMC ophthalmology. 2023 Feb 6:23(1):51. doi: 10.1186/s12886-023-02783-x. Epub 2023 Feb 6 [PubMed PMID: 36747194]
Muche N, Wasihun Y, Wondiye H, Bogale EK, Anagaw TF. Behavioral Responses for Face Cleanliness Message to Prevent Trachoma Among Mothers Having Children Age 1-9 Years Old, in Fogera District, Northwest Ethiopia: An Application of Extended Parallel Process Model. International journal of general medicine. 2023:16():1927-1941. doi: 10.2147/IJGM.S412380. Epub 2023 May 19 [PubMed PMID: 37228742]
Lakew S, Asefa G, Zerdo Z. Assessment of the status of improved F&E trachoma control practices among children of agro-pastoralists in Southern Ethiopia: a mixed design survey using theory of triadic influences. BMC public health. 2023 Mar 23:23(1):556. doi: 10.1186/s12889-023-15438-9. Epub 2023 Mar 23 [PubMed PMID: 36959544]
Level 3 (low-level) evidenceGower E, Bayissasse B, Kello AB, Jesudason T. Maintaining high quality trichiasis surgery before and after trachoma elimination. Community eye health. 2023:36(120):17 [PubMed PMID: 38178827]
Level 2 (mid-level) evidenceWang LA, Lai CC. "Etiology of trichiasis/distichiasis and its management with CO2 laser ablation". Plastic and reconstructive surgery. 2023 Oct 3:():. doi: 10.1097/PRS.0000000000011107. Epub 2023 Oct 3 [PubMed PMID: 37797242]
Habtamu E, Wondie T, Gobezie W, Tadesse Z, Gashaw B, Gebeyehu A, Roberts CH, Callahan EK, Macleod D, Burton MJ. Effect of repeated epilation for minor trachomatous trichiasis on lash burden, phenotype and surgical management willingness: A cohort study. PLoS neglected tropical diseases. 2020 Dec:14(12):e0008882. doi: 10.1371/journal.pntd.0008882. Epub 2020 Dec 14 [PubMed PMID: 33315876]
Mwangi G, Courtright P, Solomon AW. National approaches to trichiasis surgical follow-up, outcome assessment and surgeon audit in trachoma-endemic countries in Africa. The British journal of ophthalmology. 2021 Jul:105(7):904-908. doi: 10.1136/bjophthalmol-2019-315777. Epub 2020 Jul 26 [PubMed PMID: 32713838]
Kreis AJ, Gower EW, Kropp M, Kello AB, Nouhoum G, Resnikoff S, Talero SL, Solomon AW. The prevention and management of postoperative trachomatous trichiasis: A systematic review. Survey of ophthalmology. 2024 Jan-Feb:69(1):93-102. doi: 10.1016/j.survophthal.2023.02.008. Epub 2023 Mar 5 [PubMed PMID: 36878359]
Level 1 (high-level) evidenceHailemariam B, Sata E, Halefom M, Deathe AR, Zerihun M, Jensen KA, Callahan EK, Beyene M, Adriaensen W, Owiti P, Senkoro M, Zolfo M, Nash SD. Surgical output within the Fast Track Initiative against trachoma in Amhara region, Ethiopia. Journal of infection in developing countries. 2022 Aug 31:16(8.1):8S-14S. doi: 10.3855/jidc.15978. Epub 2022 Aug 31 [PubMed PMID: 36156496]
Muthiah S, Radhakrishnan N. Management of Extraocular Infections. Indian journal of pediatrics. 2017 Dec:84(12):945-952. doi: 10.1007/s12098-017-2409-y. Epub 2017 Jul 14 [PubMed PMID: 28707045]
Thylefors B, Dawson CR, Jones BR, West SK, Taylor HR. A simple system for the assessment of trachoma and its complications. Bulletin of the World Health Organization. 1987:65(4):477-83 [PubMed PMID: 3500800]
Ngondi J, Onsarigo A, Matthews F, Reacher M, Brayne C, Baba S, Solomon AW, Zingeser J, Emerson PM. Effect of 3 years of SAFE (surgery, antibiotics, facial cleanliness, and environmental change) strategy for trachoma control in southern Sudan: a cross-sectional study. Lancet (London, England). 2006 Aug 12:368(9535):589-95 [PubMed PMID: 16905023]
Level 2 (mid-level) evidenceAsmare ZA, Assefa NL, Abebe D, Nigatu SG, Alimaw YA. Trachoma prevention practice and associated factors among mothers having children aged under nine years in Andabet district, northwest Ethiopia, 2022: A multi-level analysis. PLoS neglected tropical diseases. 2023 Jun:17(6):e0011433. doi: 10.1371/journal.pntd.0011433. Epub 2023 Jun 30 [PubMed PMID: 37390045]
Ciciriello AM, Addiss DG, Teferi T, Emerson PM, Hooper PJ, Seid M, Tadesse G, Seife F, Sormolo MJ, Kebede F, Kiflu G, West SK, Alemu M, LaCon G, Gebre T. An observational assessment of the safety of mass drug administration for trachoma in Ethiopian children. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2022 Oct 2:116(10):917-923. doi: 10.1093/trstmh/trac006. Epub [PubMed PMID: 35106593]
. WHO Alliance for the Global Elimination of Trachoma by 2020: progress report on elimination of trachoma, 2014–2016. Releve epidemiologique hebdomadaire. 2017 Jun 30:92(26):359-68 [PubMed PMID: 28664685]
Larkin HD. WHO Program May Eliminate Active Trachoma's Blindness Risk by 2030. JAMA. 2022 May 17:327(19):1859. doi: 10.1001/jama.2022.7383. Epub [PubMed PMID: 35579636]
Mahmud H, Landskroner E, Amza A, Aragie S, Godwin WW, de Hostos Barth A, O'Brien KS, Lietman TM, Oldenburg CE. Stopping azithromycin mass drug administration for trachoma: A systematic review. PLoS neglected tropical diseases. 2021 Jul:15(7):e0009491. doi: 10.1371/journal.pntd.0009491. Epub 2021 Jul 8 [PubMed PMID: 34237074]
Level 1 (high-level) evidenceAstale T, Ebert CD, Nute AW, Zerihun M, Gessese D, Melak B, Sata E, Ayele Z, Ayenew G, Callahan EK, Haile M, Zeru T, Tadesse Z, Nash SD. The population-based prevalence of trachomatous scarring in a trachoma hyperendemic setting: results from 152 impact surveys in Amhara, Ethiopia. BMC ophthalmology. 2021 May 13:21(1):213. doi: 10.1186/s12886-021-01972-w. Epub 2021 May 13 [PubMed PMID: 33985443]
Level 3 (low-level) evidenceWu TJ, Reynolds MM. Trachoma, the world's leading infectious cause of blindness: The remaining gap in care and access to basic handwashing facilities. European journal of ophthalmology. 2023 Jul:33(4):1576-1582. doi: 10.1177/11206721231154295. Epub 2023 Feb 1 [PubMed PMID: 36726295]